

Mullerian duct anomalies: from diagnosis to intervention
- PMID: 19433480
- PMCID: PMC3473390
- DOI: 10.1259/bjr/99354802
Mullerian duct anomalies: from diagnosis to intervention
Abstract
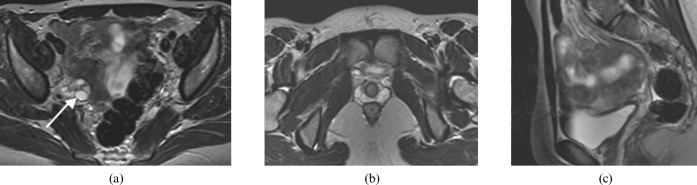
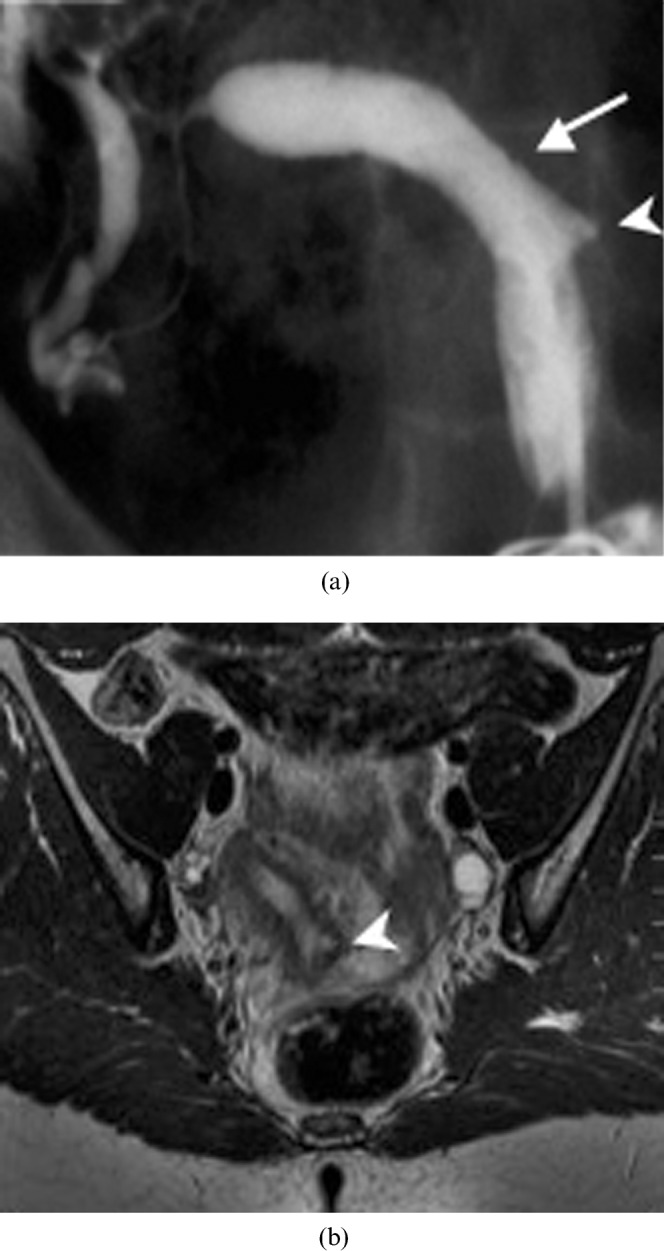
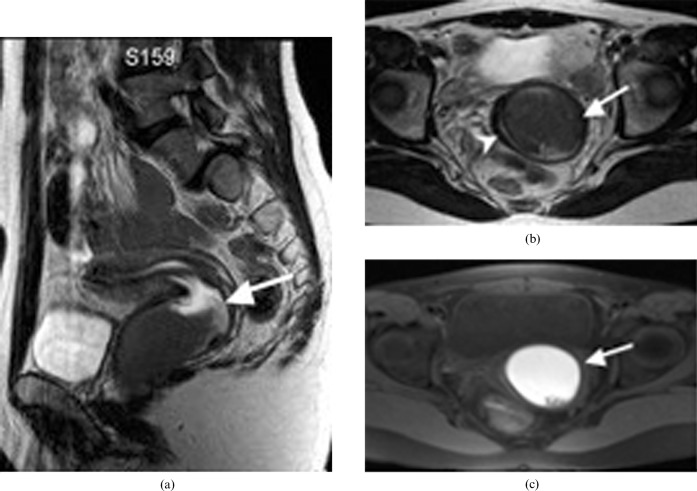
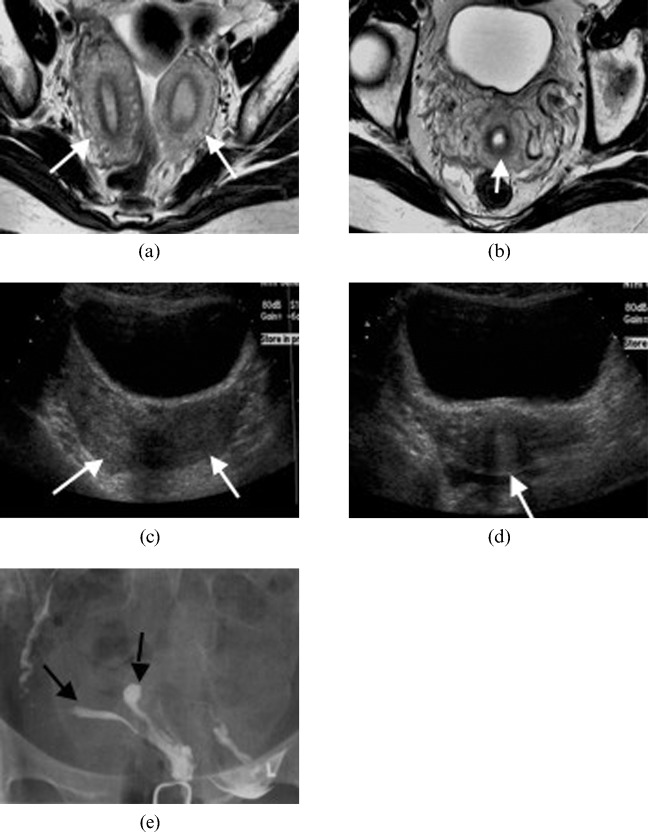
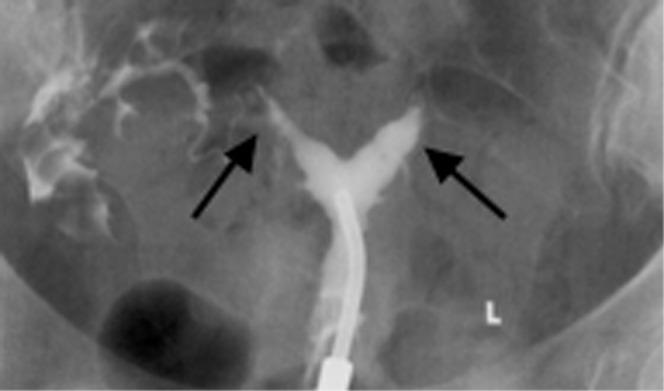
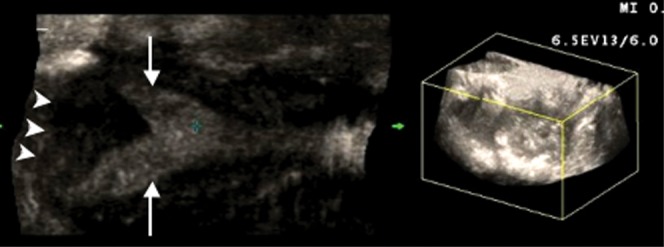
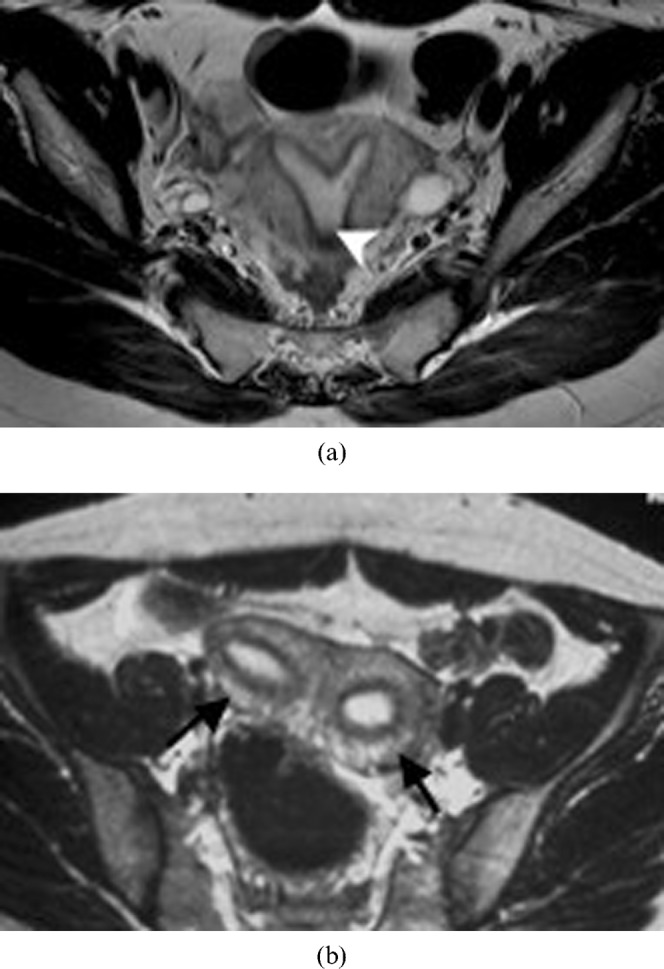
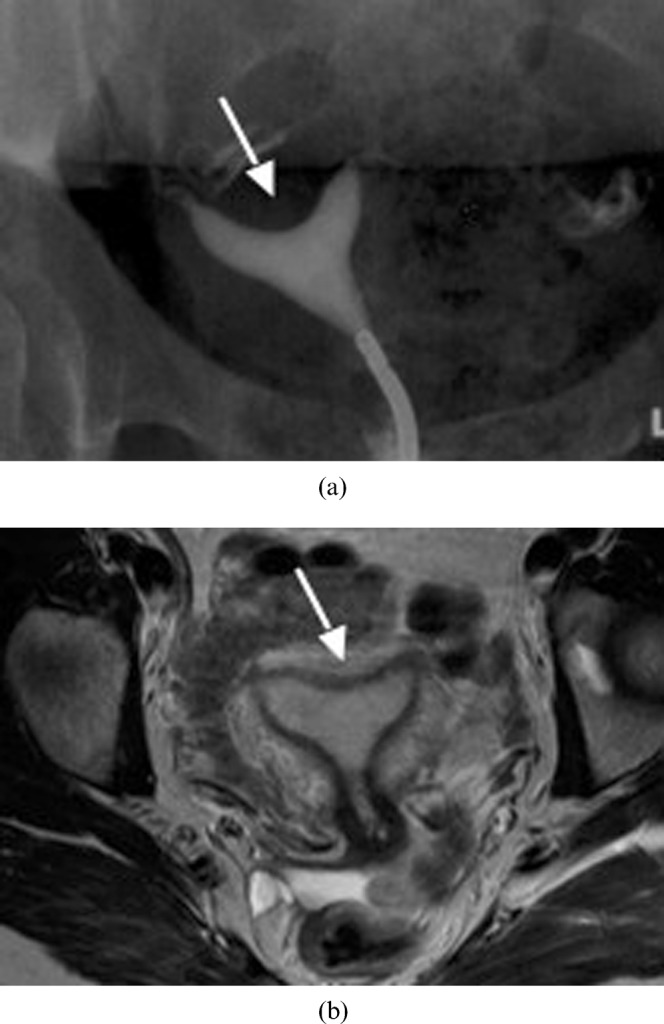
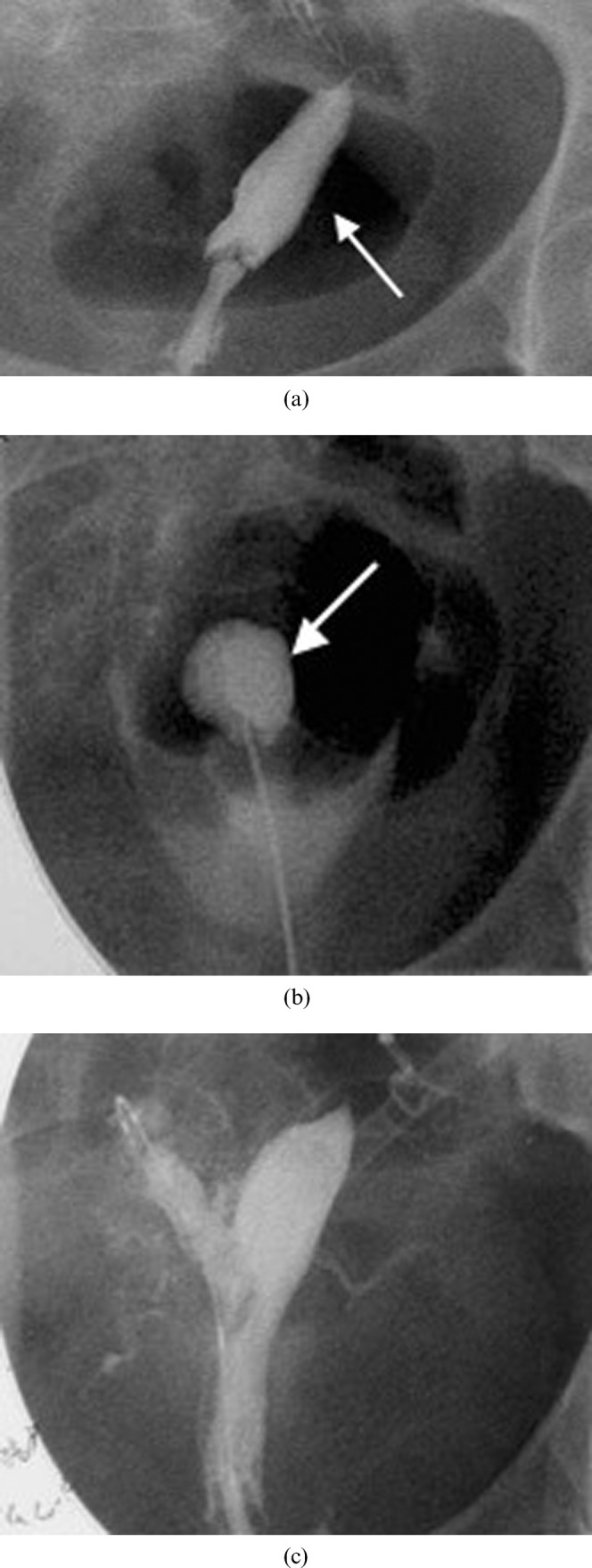
The purpose of this study was to review the embryology, classification, imaging features and treatment options of Müllerian duct anomalies. The three embryological phases will be described and the appearance of the seven classes of Müllerian duct anomalies will be illustrated using hysterosalpingography, ultrasound and MRI. This exhibit will also review the treatment options, including interventional therapy. The role of imaging is to help detect, classify and guide surgical management. At this time, MRI is the modality of choice because of its high accuracy in detecting and accurately characterising Müllerian duct anomalies. In conclusion, radiologists should be familiar with the imaging features of the seven classes of Müllerian duct anomalies, as the appropriate course of treatment relies upon the correct diagnosis and categorisation of each anomaly.
Figures





References
-
- The American Fertility Society classifications of adnexal adhesions, distal tubal obstruction, tubal occlusions secondary to tubal ligation, tubal pregnancies, Müllerian anomalies and intrauterine adhesions. Fertil Steril 1998;49:944–55 - PubMed
-
- Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of Müllerian duct anomalies. J Ultrasound Med 2008;27:413–23 - PubMed
-
- Mueller GC, Hussain HK, Smith YR, Quint EH, Carlos RC, Johnson TD, et al. Müllerian duct anomalies: comparison of MRI diagnosis and clinical diagnosis. AJR Am J Roentgenol. 2007;189:1294–302 - PubMed
-
- Heinonen PK, Saarikoski S, Pystynen P. Reproductive performance of women with uterine anomalies: an evaluation of 182 cases. Acta Obstet Gynecol Scand 1982;61:157–62 - PubMed
-
- Homer HA, Li TC, Cooke ID. The septate uterus: a review of management and reproductive outcome. Fertil Steril 2000;73:1–14 - PubMed
