

Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study
- PMID: 19436026
- PMCID: PMC2684554
- DOI: 10.1093/jnci/djp089
Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study
Abstract
Background: Information on the long-term risk of cervical intraepithelial neoplasia (CIN) recurrence among women treated for CIN is limited yet critical for evidence-based surveillance recommendations.
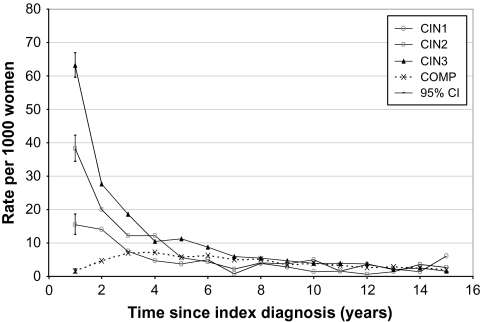
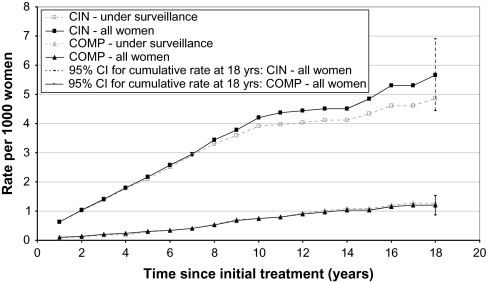
Methods: We retrospectively identified 37,142 women treated for CIN 1, 2, or 3 from January 1, 1986, through December 31, 2000 (CIN cohort), from the British Columbia Cancer Agency cytology database and linked their records with cancer registry and vital statistics data. Treatment included cryotherapy, loop electrosurgical excision procedure, cone biopsy, and laser vaporization or excision. A comparison cohort contained 71,213 women with normal cytology and no previous CIN diagnosis. Follow-up continued through December 31, 2004. Among women in both cohorts under active surveillance, we compared rates of CIN 2 or 3 (CIN 2/3) and cervical cancer. Cumulative incidence rates of CIN 2/3 and 95% confidence intervals (CIs) were estimated by a life table approach by using annual rates. Cumulative rates of invasive cancer were examined by the person-years method.
Results: Overall observed cumulative rates of CIN 2/3 in the first 6 years after treatment were 14.0% (95% CI = 13.84% to 14.15%) for women originally treated for CIN 3, 9.3% (95% CI = 9.09% to 9.42%) for CIN 2, and 5.6% (95% CI = 4.91% to 5.21%) for CIN 1. Annual rates of CIN 2/3 were less than 1% after 6 years. Initial diagnosis, age, and treatment type were associated with a diagnosis of CIN 2/3 after treatment, with 6-year adjusted rates for women aged 40-49 years ranging from 2.6% (95% CI = 1.9% to 3.4%) for treatment of CIN 1 with the loop electrosurgical excision procedure to 34.0% (95% CI = 30.9% to 37.1%) for treatment of CIN 3 with cryotherapy. Overall incidence of invasive cancer (per 100,000 woman-years) was higher in the CIN cohort (37 invasive cancers, 95% CI = 30.6 to 42.5 cancers) than in the comparison cohort (six cancers, 95% CI = 4.3 to 7.7 cancers). Cryotherapy, compared with other treatments, was associated with the highest rate of subsequent disease (adjusted odds ratio for invasive cancer = 2.98, 95% CI = 2.09 to 4.60).
Conclusion: Risk of CIN 2/3 after treatment was associated with initial CIN grade, treatment type, and age. Long-term risk of invasive cancer remained higher among women treated for CIN, particularly those treated with cryotherapy.
Figures
Comment in
-
Women with cervical intraepithelial neoplasia: requirement for active long-term surveillance after therapy.J Natl Cancer Inst. 2009 May 20;101(10):696-7. doi: 10.1093/jnci/djp097. Epub 2009 May 12. J Natl Cancer Inst. 2009. PMID: 19436033 No abstract available.
-
Re: Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study.J Natl Cancer Inst. 2009 Oct 21;101(20):1429-30. doi: 10.1093/jnci/djp307. Epub 2009 Sep 4. J Natl Cancer Inst. 2009. PMID: 19734521 Free PMC article. No abstract available.
References
-
- Woolf SH. Screening for cervical cancer. In: Goldbloom RB, Lawrence RS, editors. Preventing Disease: Beyond the Rhetoric. New York, NY: Springer Verlag; 1990. pp. 319–323.
-
- Surveillance, Epidemiology, and End Results (SEER) Program. National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch; SEER*Stat Database: Incidence–SEER 17 Regs Limited-Use, Nov 2006 Sub (1973–2004 varying) Released April 2007, based on the November 2006 submission. Available at: www.seer.cancer.gov.
-
- Kyrgiou M, Tsoumpou I, Vredoussis T, et al. Management of minor cervical abnormalities: a systematic review and a meta-analysis of the literature. Cancer Treat Rev. 2006;32(6):515–523. - PubMed
-
- The ASCUS-LSIL Triage Study (ALTS) Group. Results of a randomized trial on the management of cytology interpretations of atypical squamous cells of undetermined significance. Am J Obstet Gynecol. 2003;188(6):1383–1392. - PubMed
-
- The ASCUS-LSIL Triage Study (ALTS) Group. A randomized trial on the management of low-grade squamous intraepithelial lesion cytology interpretations. Am J Obstet Gynecol. 2003;188(6):1393–1400. - PubMed
