

Cisplatin-based chemotherapy for advanced seminoma: report of 52 cases treated in two institutions
- PMID: 19437039
- PMCID: PMC12160265
- DOI: 10.1007/s00432-009-0596-2
Cisplatin-based chemotherapy for advanced seminoma: report of 52 cases treated in two institutions
Abstract
Introduction: We evaluated an intensified therapeutic strategy in order to optimize treatment outcomes while maintaining acceptable toxicity in patients with advanced seminoma.
Patients and methods: Fifty-two patients with advanced pure seminoma were retrospectively evaluated. Patients with low-risk advanced seminoma, according to the International Germ Cell Cancer Collaborative Group Consensus Classification criteria, had received four cycles of the BEP regimen either in the 5-day or the alternative 3-day schedule, while patients with intermediate-risk advanced seminoma had received four cycles of the IBEP regimen.
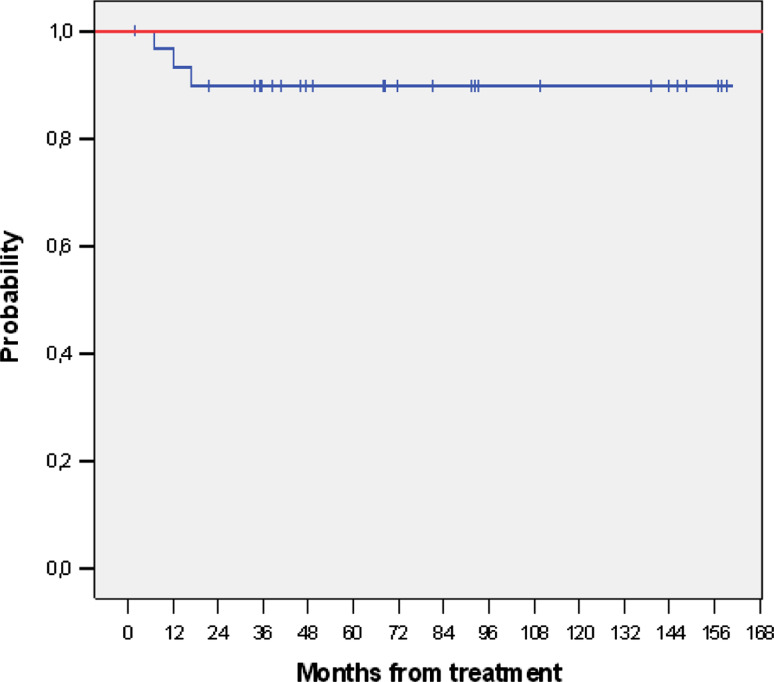
Results: Forty-two patients (80.7%) had testicular seminoma while ten patients (19.3%) presented with primary extragonadal (mediastinal or retroperitoneal) tumor. Forty-seven (90.8%) patients belonged to the low-risk group and five patients (9.2%) to the intermediate-risk group. Treatment-related toxicity was moderate, with febrile neutropenia being the most prevalent (13.5%). Twenty patients (38.5%) achieved a complete response to chemotherapy. Twenty-three from the remaining 32 patients had residual masses more than 3 cm and were submitted to surgery (2 patients), FDG-PET scan (8 patients) or surveillance (13 patients). After 69 months of follow-up there were three recurrences that were successfully treated with high-dose or salvage chemotherapy. No death by any cause was recorded.
Conclusions: Intensified cisplatin-based chemotherapy for patients with advanced seminoma does not confer evidence of superiority over radiotherapy alone or the standard BEP regimen. Patients with low-volume abdominal disease (clinical stage IIA and IIB) can be cured by four cycles of BEP instead of radiotherapy at the cost of a substantial increase in chemotherapy exposure and the resulting toxicity.
Figures
References
-
- Cancer Therapy Evaluation Program (2003), Common Terminology Criteria for Adverse Events v4.0 (CTCAE), March 31, 2003 (http://ctep.cancer.gov)
-
- Cullen M, Harper G, Woodroffe et al (1988) Chemotherapy for poor risk germ cell tumours. An independent evaluation of the POMB/ACE regime. Br J Urol 62(5):454–460. doi:10.1111/j.1464-410X.1988.tb04396.x - PubMed
-
- De Santis M, Bokemeyer C, Becherer A et al (2001) Predictive impact of 2–18fluoro-2-deoxy-D-glucose positron emission tomography for residual postchemotherapy masses in patients with bulky seminoma. J Clin Oncol 19(17):3740–3744 - PubMed
-
- De Wit R, Roberts J, Wilkinson P et al (2001) Equivalence of three or four cycles of bleomycin, etoposide, and cisplatin chemotherapy and of a 3- or 5-day schedule in good-prognosis germ cell cancer: a randomized study of the European Organization for Research and Treatment of Cancer Genitourinary Tract Cancer Cooperative Group and the Medical Research Council. J Clin Oncol 19(6):1629–1640 - PubMed
-
- Fossa S, de Wit R, Roberts T et al (2003) Quality of life in good prognosis patients with metastatic germ cell cancer: a prospective study of the European Organization for Research and Treatment of Cancer Genitourinary Group/Medical Research Council Testicular Cancer Study Group (30941/TE20). J Clin Oncol 21(6):1107–1118. doi:10.1200/JCO.2003.02.075 - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
