

Adjuvant chemotherapy in older women with early-stage breast cancer
- PMID: 19439741
- PMCID: PMC3082436
- DOI: 10.1056/NEJMoa0810266
Adjuvant chemotherapy in older women with early-stage breast cancer
Erratum in
- N Engl J Med. 2009 Oct 22;361(17):1714. Magrinat, Gutav [corrected to Magrinat, Gustav]
Abstract
Background: Older women with breast cancer are underrepresented in clinical trials, and data on the effects of adjuvant chemotherapy in such patients are scant. We tested for the noninferiority of capecitabine as compared with standard chemotherapy in women with breast cancer who were 65 years of age or older.
Methods: We randomly assigned patients with stage I, II, IIIA, or IIIB breast cancer to standard chemotherapy (either cyclophosphamide, methotrexate, and fluorouracil or cyclophosphamide plus doxorubicin) or capecitabine. Endocrine therapy was recommended after chemotherapy in patients with hormone-receptor-positive tumors. A Bayesian statistical design was used with a range in sample size from 600 to 1800 patients. The primary end point was relapse-free survival.
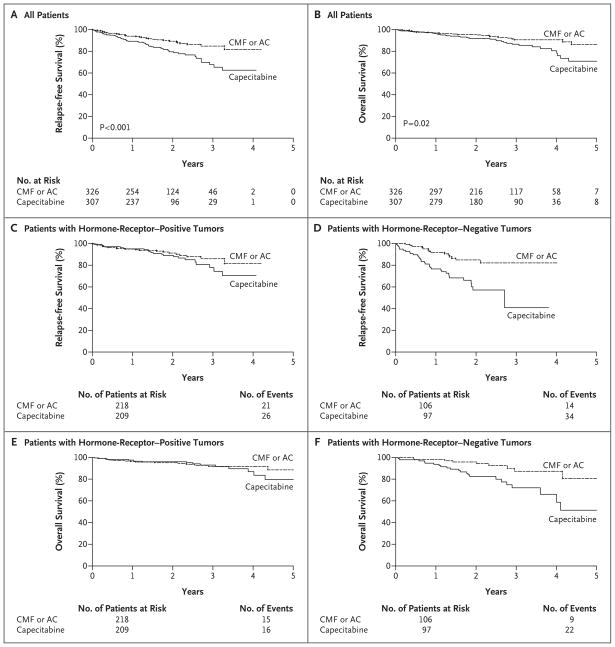
Results: When the 600th patient was enrolled, the probability that, with longer follow-up, capecitabine therapy was highly likely to be inferior to standard chemotherapy met a prescribed level, and enrollment was discontinued. After an additional year of follow-up, the hazard ratio for disease recurrence or death in the capecitabine group was 2.09 (95% confidence interval, 1.38 to 3.17; P<0.001). Patients who were randomly assigned to capecitabine were twice as likely to have a relapse and almost twice as likely to die as patients who were randomly assigned to standard chemotherapy (P=0.02). At 3 years, the rate of relapse-free survival was 68% in the capecitabine group versus 85% in the standard-chemotherapy group, and the overall survival rate was 86% versus 91%. Two patients in the capecitabine group died of treatment-related complications; as compared with patients receiving capecitabine, twice as many patients receiving standard chemotherapy had moderate-to-severe toxic effects (64% vs. 33%).
Conclusions: Standard adjuvant chemotherapy is superior to capecitabine in patients with early-stage breast cancer who are 65 years of age or older. (ClinicalTrials.gov number, NCT00024102.)
2009 Massachusetts Medical Society
Conflict of interest statement
Drs. Muss, Berry, Norton, and Hudis report receiving consulting fees from Hoffmann-La Roche; and Drs. Gralow, Hudis, Wolff, and Perez, research support from Hoffman-La Roche. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Adjuvant chemotherapy for older adults with breast cancer: making the standard a standard.Womens Health (Lond). 2009 Sep;5(5):481-4. doi: 10.2217/whe.09.43. Womens Health (Lond). 2009. PMID: 19702447 Review.
-
Chemotherapy in older women with breast cancer.N Engl J Med. 2009 Sep 3;361(10):1023; author reply 1023-4. doi: 10.1056/NEJMc091265. N Engl J Med. 2009. PMID: 19726778 No abstract available.
-
Chemotherapy in older women with breast cancer.N Engl J Med. 2009 Sep 3;361(10):1023; author reply 1023-4. N Engl J Med. 2009. PMID: 19731412 No abstract available.
References
-
- [Accessed April 21, 2009];Surveillance Epidemiology and End Results cancer statistics review. at http://seer.cancer.gov/csr/1975_2005/results_merged/sect_04_breast.pdf.
-
- Hébert-Croteau N, Brisson J, Latreille J, Blanchette C, Deschênes L. Compliance with consensus recommendations for the treatment of early stage breast carcinoma in elderly women. Cancer. 1999;85:1104–13. - PubMed
-
- Yancik R, Wesley MN, Ries LA, Havlik RJ, Edwards BK, Yates JW. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA. 2001;285:885–92. - PubMed
-
- Wildiers H, Kunkler I, Biganzoli L, et al. Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology. Lancet Oncol. 2007;8:1101–15. - PubMed
-
- Hébert-Croteau N, Brisson J, Latreille J, Rivard M, Abdelaziz N, Martin G. Compliance with consensus recommendations for systemic therapy is associated with improved survival of women with node-negative breast cancer. J Clin Oncol. 2004;22:3685–93. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous