

The abdominal circulatory pump
- PMID: 19440240
- PMCID: PMC2678249
- DOI: 10.1371/journal.pone.0005550
The abdominal circulatory pump
Abstract
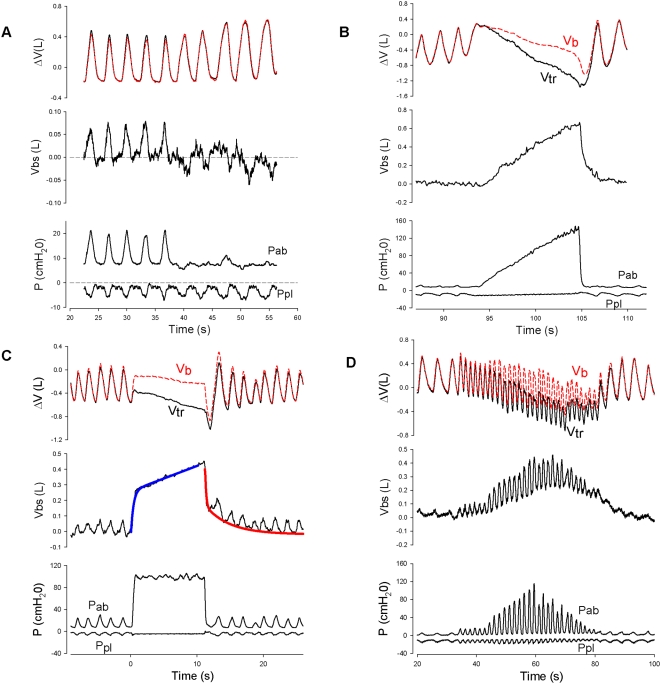
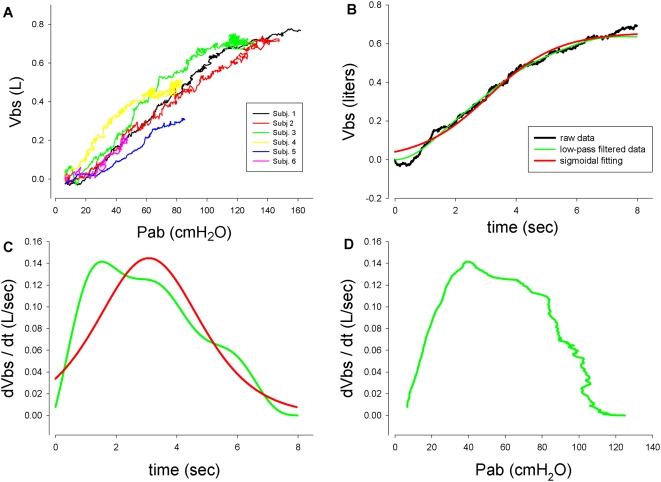
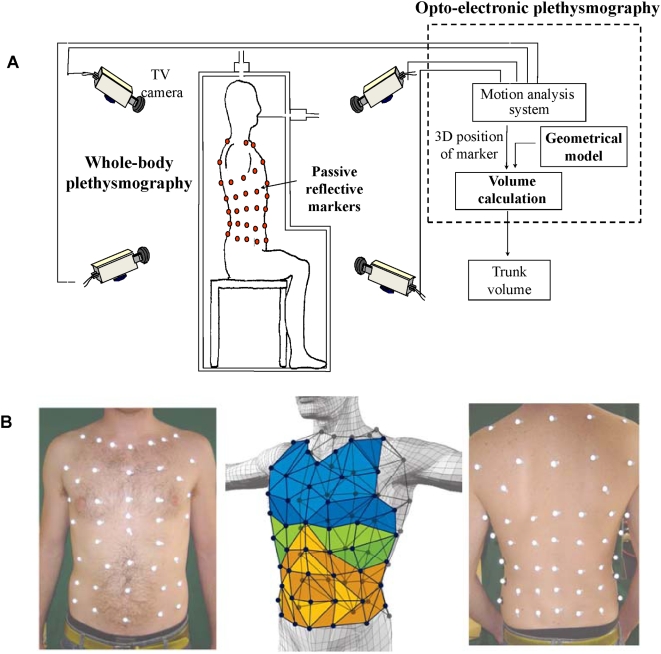
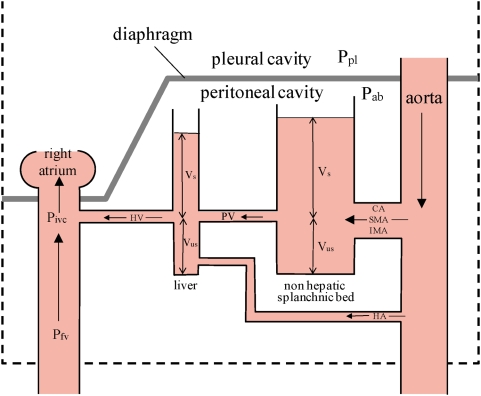
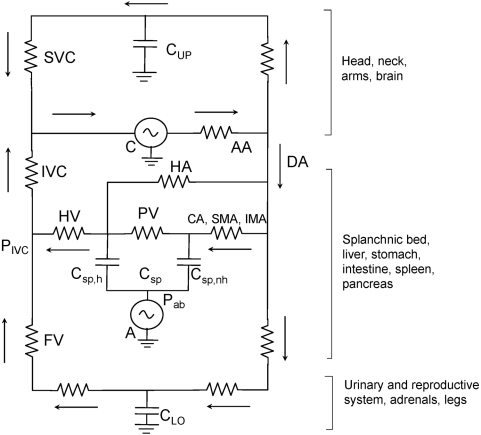
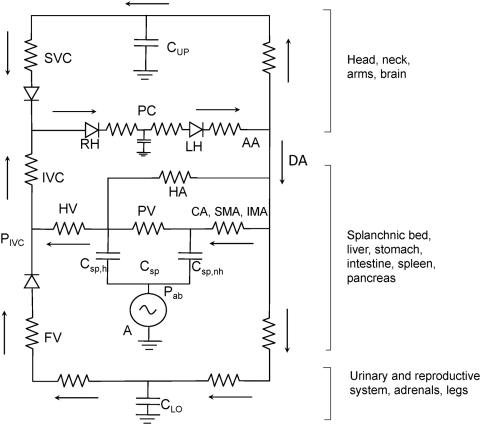
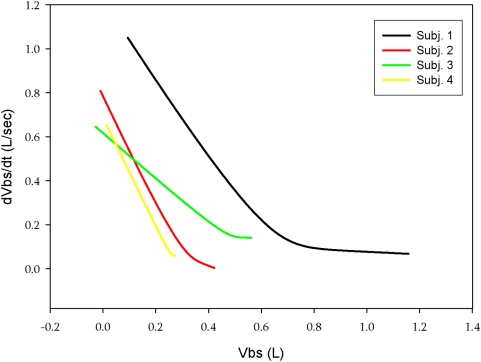
Blood in the splanchnic vasculature can be transferred to the extremities. We quantified such blood shifts in normal subjects by measuring trunk volume by optoelectronic plethysmography, simultaneously with changes in body volume by whole body plethysmography during contractions of the diaphragm and abdominal muscles. Trunk volume changes with blood shifts, but body volume does not so that the blood volume shifted between trunk and extremities (Vbs) is the difference between changes in trunk and body volume. This is so because both trunk and body volume change identically with breathing and gas expansion or compression. During tidal breathing Vbs was 50-75 ml with an ejection fraction of 4-6% and an output of 750-1500 ml/min. Step increases in abdominal pressure resulted in rapid emptying presumably from the liver with a time constant of 0.61+/-0.1SE sec. followed by slower flow from non-hepatic viscera. The filling time constant was 0.57+/-0.09SE sec. Splanchnic emptying shifted up to 650 ml blood. With emptying, the increased hepatic vein flow increases the blood pressure at its entry into the inferior vena cava (IVC) and abolishes the pressure gradient producing flow between the femoral vein and the IVC inducing blood pooling in the legs. The findings are important for exercise because the larger the Vbs the greater the perfusion of locomotor muscles. During asystolic cardiac arrest we calculate that appropriate timing of abdominal compression could produce an output of 6 L/min. so that the abdominal circulatory pump might act as an auxiliary heart.
Conflict of interest statement
Figures

References
-
- Iandelli I, Aliverti A, Kayser B, Dellacà R, Cala SJ, et al. Determinants of exercise performance in normal men with externally imposed expiratory flow limitation. J Appl Physiol. 2002;92:1943–1952. - PubMed
-
- Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, et al. Chest wall and lung volume estimation by optical reflectance motion analysis. J.Appl.Physiol. 1996;81:2680–2689. - PubMed
-
- Aliverti A, Dellacà RL, Lotti P, Bertini S, Duranti R, et al. Influence of expiratory flow-limitation during exercise on systemic oxygen delivery in humans. Eur J Appl Physiol. 2005;95:229–242. - PubMed
-
- Criley JM, Blaufuss AH, Kissel GL. Cough-induced cardiac compression. Self-administered from of cardiopulmonary resuscitation. JAMA. 1976;236:1246–1250. - PubMed
-
- Niemann JT, Rosborough J, Hausknecht M, Brown D, Criley JM. Cough-CPR: Documentation of systemic perfusion in man and in an experimental model: a “window” to the mechanism of blood flow in external CPR. Crit Care Med. 1980;8:141–146. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
