

Current practice of abdominal wall closure in elective surgery - Is there any consensus?
- PMID: 19442311
- PMCID: PMC2687428
- DOI: 10.1186/1471-2482-9-8
Current practice of abdominal wall closure in elective surgery - Is there any consensus?
Abstract
Background: Development of incisional hernia after open abdominal surgery remains a major cause of post-operative morbidity. The aim of this study was to determine the current practice of surgeons in terms of access to and closure of the abdominal cavity in elective open surgery.
Methods: Twelve surgical departments of the INSECT-Trial group documented the following variables for 50 consecutive patients undergoing abdominal surgery: fascial closure techniques, applied suture materials, application of subcutaneous sutures, subcutaneous drains, methods for skin closure. Descriptive analysis was performed and consensus of treatment variables was categorized into four levels: Strong consensus >95%, consensus 75-95%, overall agreement 50-75%, no consensus <50%.
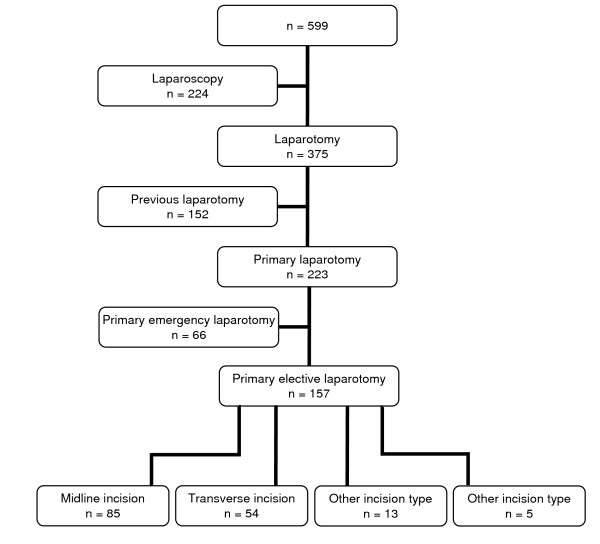
Results: 157 out of 599 patients were eligible for analysis (85 (54%) midline, 54 (35%) transverse incisions). After midline incisions the fascia was closed continuously in 55 patients (65%), using slowly absorbable (n = 47, 55%), braided (n = 32, 38%) sutures with a strength of 1 (n = 48, 57%). In the transverse setting the fascia was closed continuously in 39 patients (72%) with slowly absorbable (n = 22, 41%) braided sutures (n = 27, 50%) with a strength of 1 (n = 30, 56%).
Conclusion: In the present evaluation midline incision was the most frequently applied access in elective open abdominal surgery. None of the treatments for abdominal wall closure (except skin closure in the midline group) is performed on a consensus level.
Figures
References
-
- Israelsson LA, Jonsson T. Incisional hernia after midline laparotomy: a prospective study. Eur J Surg. 1996;162:125–129. - PubMed
-
- Gislason H, Gronbech JE, Soreide O. Burst abdomen and incisional hernia after major gastrointestinal operations – comparison of three closure techniques. Eur J Surg. 1995;161:349–354. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
