

DYNC2H1 mutations cause asphyxiating thoracic dystrophy and short rib-polydactyly syndrome, type III
- PMID: 19442771
- PMCID: PMC2681009
- DOI: 10.1016/j.ajhg.2009.04.016
DYNC2H1 mutations cause asphyxiating thoracic dystrophy and short rib-polydactyly syndrome, type III
Abstract
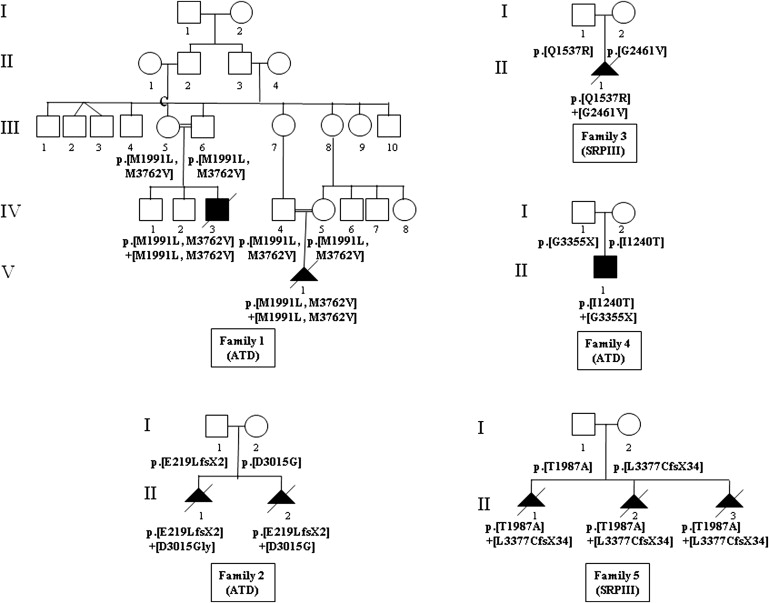
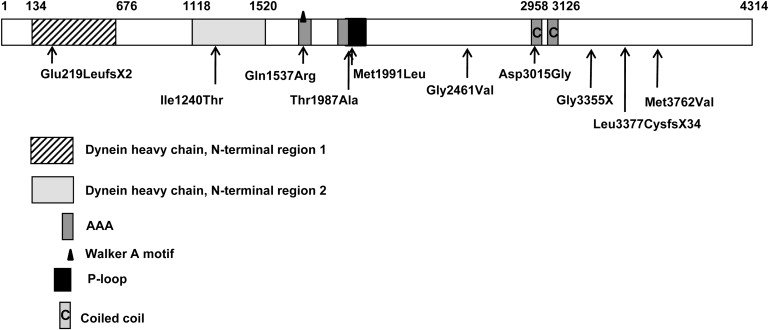
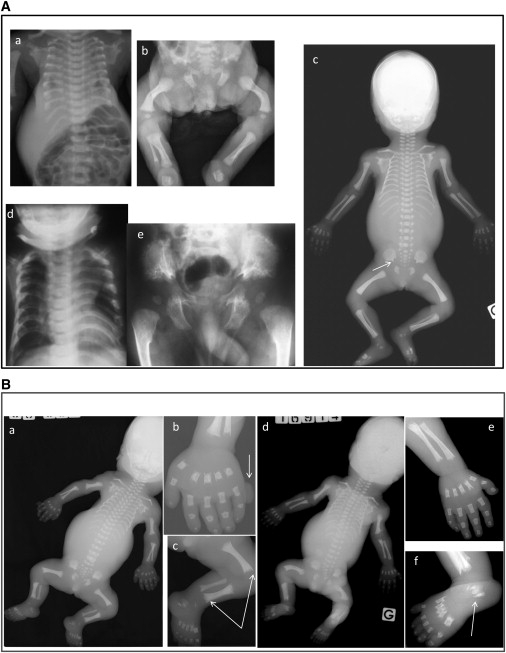
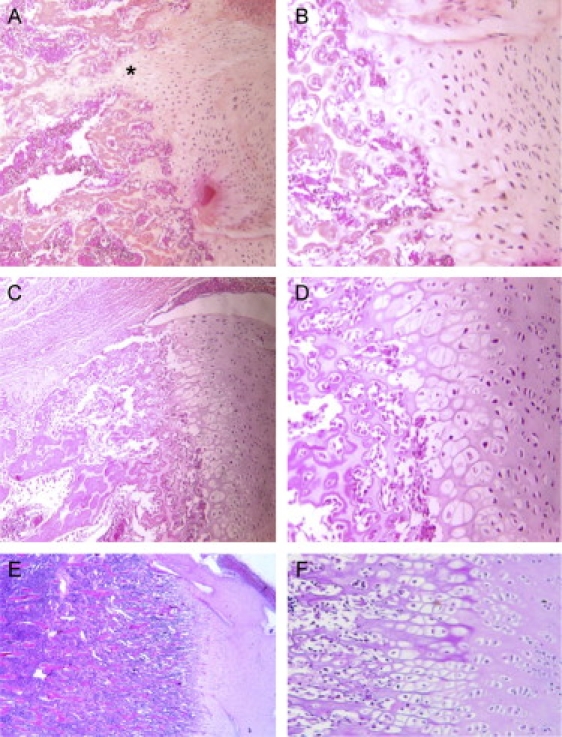
Jeune asphyxiating thoracic dystrophy (ATD) is an autosomal-recessive chondrodysplasia characterized by short ribs and a narrow thorax, short long bones, inconstant polydactyly, and trident acetabular roof. ATD is closely related to the short rib polydactyly syndrome (SRP) type III, which is a more severe condition characterized by early prenatal expression and lethality and variable malformations. We first excluded IFT80 in a series of 26 fetuses and children belonging to 14 families diagnosed with either ATD or SRP type III. Studying a consanguineous family from Morocco, we mapped an ATD gene to chromosome 11q14.3-q23.1 in a 20.4 Mb region and identified homozygous mutations in the cytoplasmic dynein 2 heavy chain 1 (DYNC2H1) gene in the affected children. Compound heterozygosity for DYNC2H1 mutations was also identified in four additional families. Among the five families, 3/5 were diagnosed with ATD and 2/5 included pregnancies terminated for SRP type III. DYNC2H1 is a component of a cytoplasmic dynein complex and is directly involved in the generation and maintenance of cilia. From this study, we conclude that ATD and SRP type III are variants of a single disorder belonging to the ciliopathy group.
Figures
References
-
- Beales P.L., Bland E., Tobin J.L., Bacchelli C., Tuysuz B., Hill J., Rix S., Pearson C.G., Kai M., Hartley J. IFT80, which encodes a conserved intraflagellar transport protein, is mutated in Jeune asphyxiating thoracic dystrophy. Nat. Genet. 2007;39:727–729. - PubMed
-
- Superti-Furga A., Unger S. Nosology and classification of genetic skeletal disorders: 2006 revision. Am. J. Med. Genet. 2007;143:1–18. - PubMed
-
- Ho N.C., Francomano C.A., van Allen M. Jeune asphyxiating thoracic dystrophy and short-rib polydactyly type III (Verma-Naumoff) are variants of the same disorder. Am. J. Med. Genet. 2000;90:310–314. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
