

F18-fluorodeoxyglucose positron emission tomography in the context of other imaging techniques and prognostic factors in multiple myeloma
- PMID: 19443657
- PMCID: PMC2744568
- DOI: 10.1182/blood-2009-03-213280
F18-fluorodeoxyglucose positron emission tomography in the context of other imaging techniques and prognostic factors in multiple myeloma
Abstract
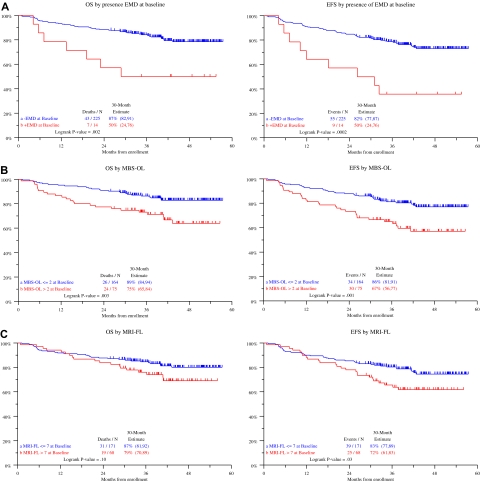
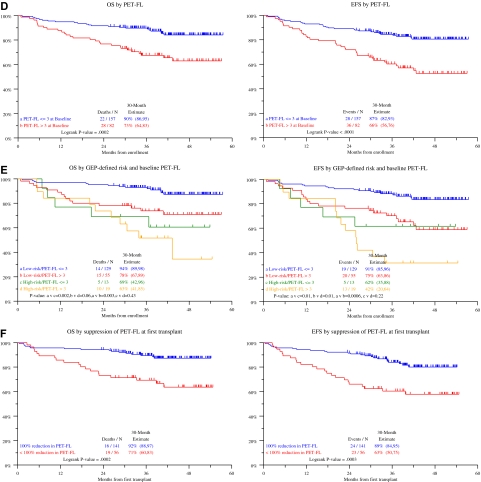
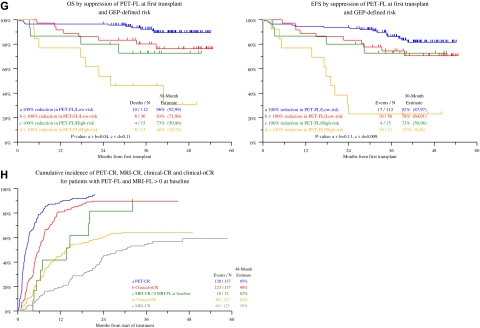
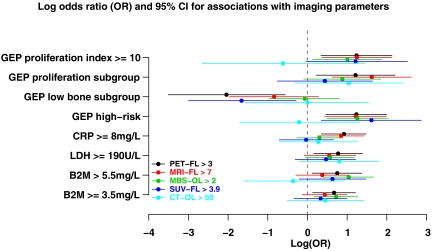
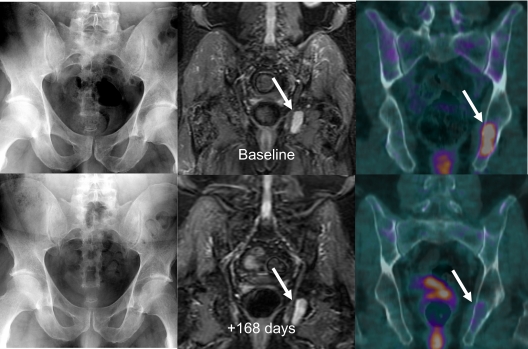
F18-fluorodeoxyglucose positron emission tomography (FDG-PET) is a powerful tool to investigate the role of tumor metabolic activity and its suppression by therapy for cancer survival. As part of Total Therapy 3 for newly diagnosed multiple myeloma, metastatic bone survey, magnetic resonance imaging, and FDG-PET scanning were evaluated in 239 untreated patients. All 3 imaging techniques showed correlations with prognostically relevant baseline parameters: the number of focal lesions (FLs), especially when FDG-avid by PET-computed tomography, was positively linked to high levels of beta-2-microglobulin, C-reactive protein, and lactate dehydrogenase; among gene expression profiling parameters, high-risk and proliferation-related parameters were positively and low-bone-disease molecular subtype inversely correlated with FL. The presence of more than 3 FDG-avid FLs, related to fundamental features of myeloma biology and genomics, was the leading independent parameter associated with inferior overall and event-free survival. Complete FDG suppression in FL before first transplantation conferred significantly better outcomes and was only opposed by gene expression profiling-defined high-risk status, which together accounted for approximately 50% of survival variability (R(2) test). Our results provide a rationale for testing the hypothesis that myeloma survival can be improved by altering treatment in patients in whom FDG suppression cannot be achieved after induction therapy.
Figures
Comment in
-
A new pet for myeloma.Blood. 2009 Sep 3;114(10):2007-8. doi: 10.1182/blood-2009-06-224196. Blood. 2009. PMID: 19729530
References
-
- Dimopoulos MA, Moulopoulos LA, Datseris I, et al. Imaging of myeloma bone disease. Acta Oncol. 2000;39:823–827. - PubMed
-
- Lecouvet FE, Van de Berg BC, Malghem J, et al. Magnetic resonance and computed tomography imaging in multiple myeloma. Semin Musculoskelet Radiol. 2001;5:43–55. - PubMed
-
- Moulopoulos LA, Varma DG, Dimopoulos MA. Multiple myeloma: spinal MR imaging in patients with untreated newly diagnosed disease. Radiology. 1992;185:833–840. - PubMed
-
- Roodman G. Mechanisms of bone metastasis. N Engl J Med. 2004;350:1655–1664. - PubMed
-
- Yaccoby S, Pearse RN, Johnson CL, et al. Myeloma interacts with the bone marrow microenvironment to induce osteoclastogenesis and is dependent on osteoclast activity. Br J Haematol. 2002;116:278–290. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
