

Microbleeds versus macrobleeds: evidence for distinct entities
- PMID: 19443797
- PMCID: PMC2758289
- DOI: 10.1161/STROKEAHA.109.548974
Microbleeds versus macrobleeds: evidence for distinct entities
Abstract
Background and purpose: Small, asymptomatic microbleeds commonly accompany larger symptomatic macrobleeds. It is unclear whether microbleeds and macrobleeds represent arbitrary categories within a single continuum versus truly distinct events with separate pathophysiologies.
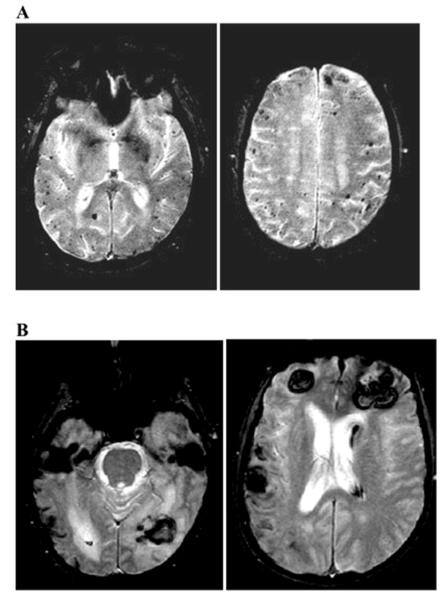
Methods: We performed 2 complementary retrospective analyses. In a radiographic analysis, we measured and plotted the volumes of all hemorrhagic lesions detected by gradient-echo MRI among 46 consecutive patients with symptomatic primary lobar intracerebral hemorrhage diagnosed as probable or possible cerebral amyloid angiopathy. In a second neuropathologic analysis, we performed blinded qualitative and quantitative examinations of amyloid-positive vessel segments in 6 autopsied subjects whose MRI scans demonstrated particularly high microbleed counts (>50 microbleeds on MRI, n=3) or low microbleed counts (<3 microbleeds, n=3).
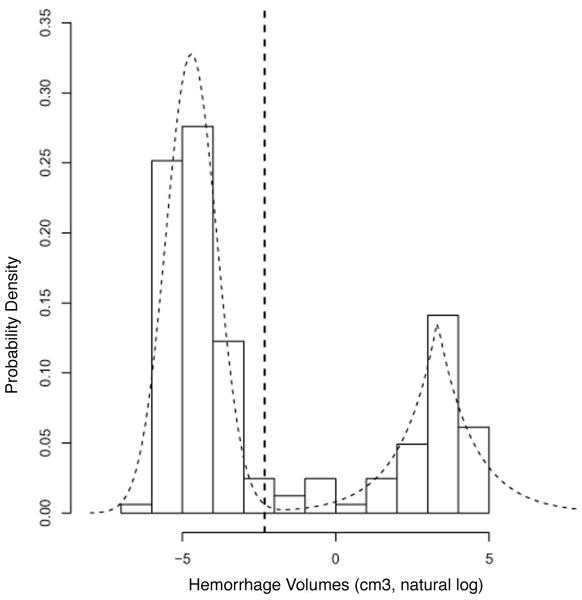
Results: Plotted on a logarithmic scale, the volumes of 163 hemorrhagic lesions identified on scans from the 46 subjects fell in a distinctly bimodal distribution with mean volumes for the 2 modes of 0.009 cm(3) and 27.5 cm(3). The optimal cut point for separating the 2 peaks (determined by receiver operating characteristics) corresponded to a lesion diameter of 0.57 cm. On neuropathologic analysis, the high microbleed-count autopsied subjects showed significantly thicker amyloid-positive vessel walls than the low microbleed-count subjects (proportional wall thickness 0.53+/-0.01 versus 0.37+/-0.01; P<0.0001; n=333 vessel segments analyzed).
Conclusions: These findings suggest that cerebral amyloid angiopathy-associated microbleeds and macrobleeds comprise distinct entities. Increased vessel wall thickness may predispose to formation of microbleeds relative to macrobleeds.
Figures

References
-
- Koennecke HC. Cerebral microbleeds on mri: Prevalence, associations, and potential clinical implications. Neurology. 2006;66:165–171. - PubMed
-
- Viswanathan A, Chabriat H. Cerebral microhemorrhage. Stroke. 2006;37:550–555. - PubMed
-
- Cordonnier C, Salman R Al-Shahi, Wardlaw J. Spontaneous brain microbleeds: Systematic review, subgroup analyses and standards for study design and reporting. Brain. 2007;130:1988–2003. - PubMed
-
- Fazekas F, Kleinert R, Roob G, Kleinert G, Kapeller P, Schmidt R, Hartung HP. Histopathologic analysis of foci of signal loss on gradient-echo t2*-weighted mr images in patients with spontaneous intracerebral hemorrhage: Evidence of microangiopathy-related microbleeds. AJNR Am J Neuroradiol. 1999;20:637–642. - PMC - PubMed
-
- Jeerakathil T, Wolf PA, Beiser A, Hald JK, Au R, Kase CS, Massaro JM, DeCarli C. Cerebral microbleeds: Prevalence and associations with cardiovascular risk factors in the framingham study. Stroke. 2004;35:1831–1835. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
