

Patent foramen ovale in cryptogenic stroke: incidental or pathogenic?
- PMID: 19443800
- PMCID: PMC2764355
- DOI: 10.1161/STROKEAHA.109.547828
Patent foramen ovale in cryptogenic stroke: incidental or pathogenic?
Abstract
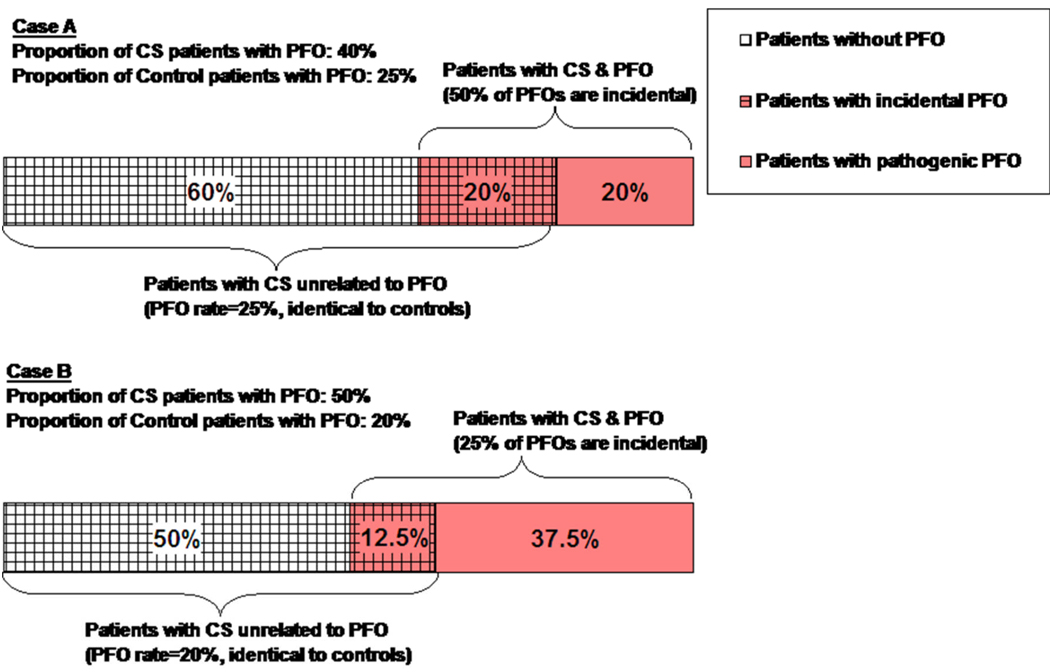
Background and purpose: Patent foramen ovale (PFO) is significantly associated with cryptogenic stroke (CS). However, even in patients with CS, a PFO can be an incidental finding. We sought to estimate the probability that a PFO in a patient with CS is incidental.
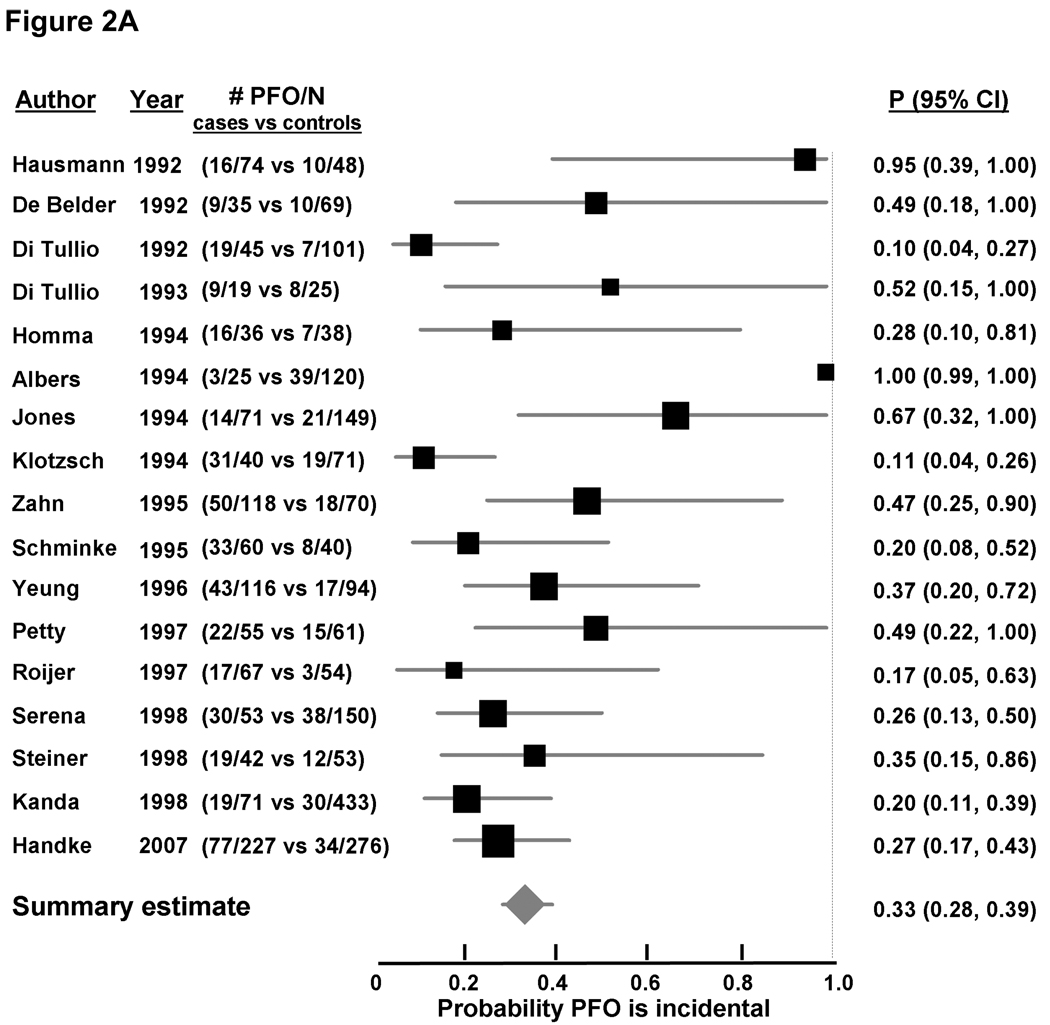
Methods: A systematic search identified 23 case-control studies examining the prevalence of PFO in patients with CS versus control subjects with stroke of known cause. Using simple assumptions and Bayes' theorem, we calculated the probability a PFO is incidental in patients with CS. Random effects meta-analyses estimated the odds ratio (OR) of a PFO in CS versus control subjects in different age populations, with or without atrial septal aneurysms, and were used to summarize across studies the probability that a PFO in CS is incidental.
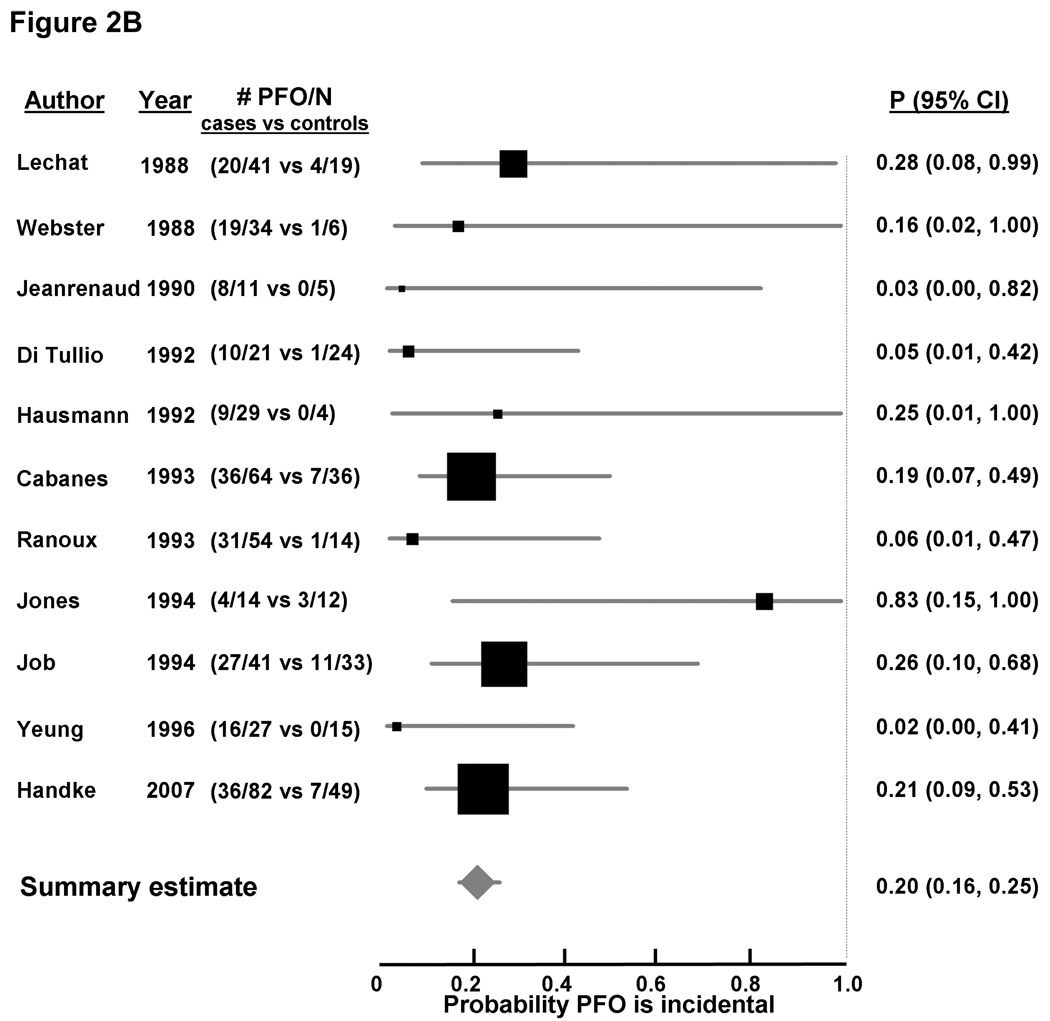
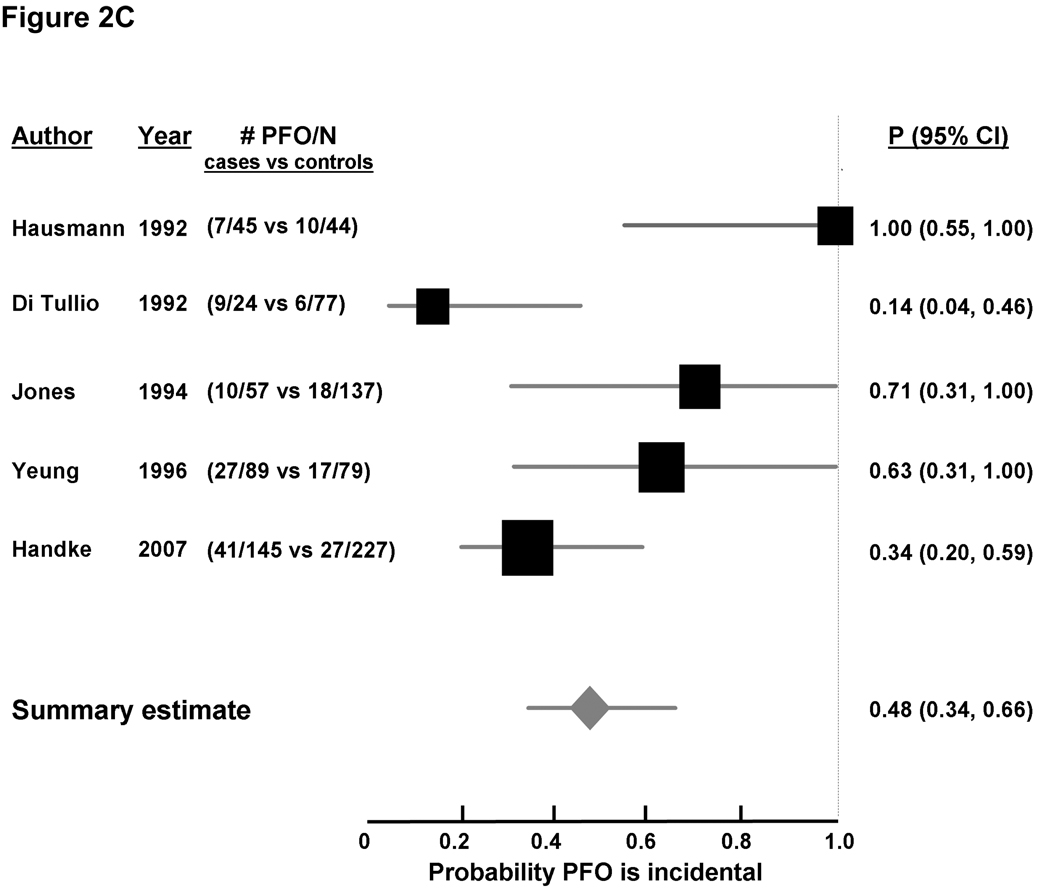
Results: The summary OR (95% CIs) for PFO in CS versus control subjects was 2.9 (CI, 2.1 to 4.0). The corresponding ORs for young and old patients (< or >or=55 years) were 5.1 (3.3 to 7.8) and 2.0 (>1.0 to 3.7), respectively. The corresponding probabilities that a PFO in patients with CS is incidental were 33% (28% to 39%) in age-inclusive studies, 20% (16% to 25%) in younger patients, and 48% (34% to 66%) in older patients. These probabilities were much lower when an atrial septal aneurysm was present.
Conclusions: In patients with otherwise CS, approximately one third of discovered PFOs are likely to be incidental and hence not benefit from closure. This probability is sensitive to patient characteristics such as age and the presence of an atrial septal aneurysm, suggesting the importance of patient selection in therapeutic decision-making.
Figures
Comment in
-
Critique of closure or medical therapy for cryptogenic stroke with patent foramen ovale: the hole truth?Stroke. 2012 Nov;43(11):3147-9. doi: 10.1161/STROKEAHA.112.659599. Epub 2012 Sep 18. Stroke. 2012. PMID: 22989503 No abstract available.
References
-
- Sacco RL, Ellenberg JH, Mohr JP, Tatemichi TK, Hier DB, Price TR, Wolf PA. Infarcts of undetermined cause: The NINCDS stroke data bank. Ann Neurol. 1989;25:382–390. - PubMed
-
- Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: A meta-analysis of case-control studies. Neurology. 2000;55:1172–1179. - PubMed
-
- Homma S, Sacco RL. Patent foramen ovale and stroke. Circulation. 2005;112:1063–1072. - PubMed
-
- Mas JL, Arquizan C, Lamy C, Zuber M, Cabanes L, Derumeaux G, Coste J. Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N Engl J Med. 2001;345:1740–1746. - PubMed
-
- Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: An autopsy study of 965 normal hearts. Mayo Clin Proc. 1984;59:17–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
