

Load sharing mechanism across graft-bone interface in static cervical locking plate fixation
- PMID: 19444346
- PMCID: PMC2682116
- DOI: 10.3340/jkns.2009.45.4.213
Load sharing mechanism across graft-bone interface in static cervical locking plate fixation
Abstract
Objective: This study is a retrospective clinical study over more than 4 years of follow up to understand the mechanism of load sharing across the graft-bone interface in the static locking plate (SLP) fixation compared with non-locking plate (NLP).
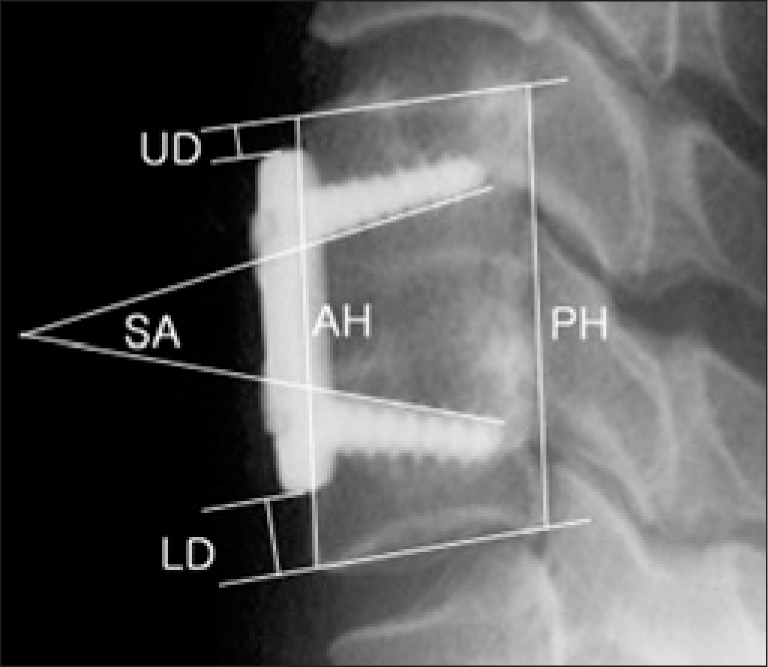
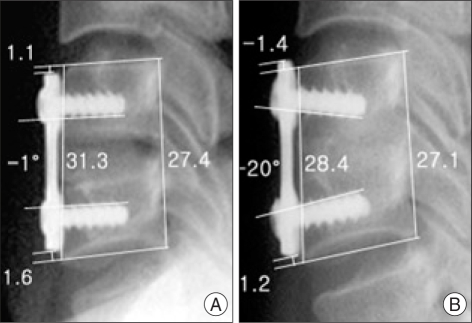
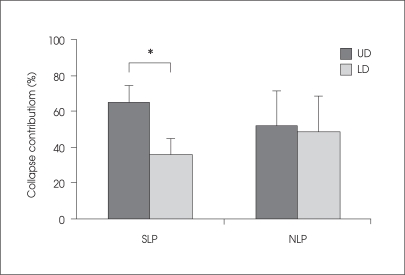
Methods: Orion locking plates and Top non-locking plates were used for SLP fixation in 29 patients and NLP fixation in 24 patients, respectively. Successful interbody fusion was estimated by dynamic X-ray films. The checking parameters were as follows : screw angle (SA) between upper and lower screw, anterior and posterior height of fusion segment between upper and lower endplate (AH & PH), and upper and lower distance from vertebral endplate to the end of plate (UD & LD). Each follow-up value of AH and PH were compared to initial values. Contributions of upper and lower collapse to whole segment collapse were estimated.
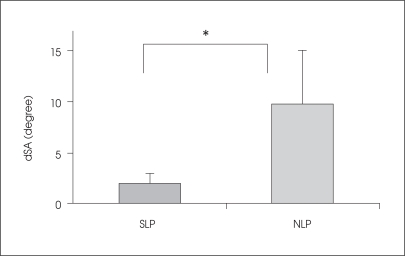
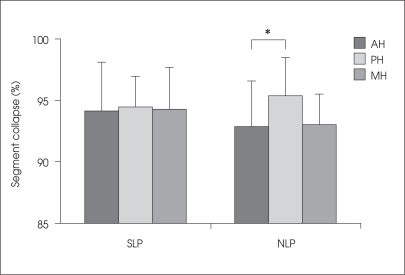
Results: Successful intervertebral bone fusion rate was 100% in the SLP group and 92% in the NLP group. The follow-up mean value of SA in SLP group was not significantly changed compared with initial value, but follow-up mean value of SA in NLP group decreased more than those in SLP group (p=0.0067). Statistical analysis did not show a significant difference in the change in AH and PH between SLP and NLP groups (p>0.05). Follow-up AH of NLP group showed more collapse than PH of same group (p=0.04). The upper portion of the vertebral body collapsed more than the lower portion in the SLP fixation (p=0.00058).
Conclusion: The fused segments with SLP had successful bone fusion without change in initial screw angle, which was not observed in NLP fixation. It suggests that there was enough load sharing across bone-graft interface in SLP fixation.
Keywords: Cervical vertebrae; Spinal fusion; Surgical Fixation Devices.
Figures

Similar articles
-
The effect of locking fixation screws on the stability of anterior cervical plating.Spine (Phila Pa 1976). 1999 Feb 15;24(4):334-8. doi: 10.1097/00007632-199902150-00005. Spine (Phila Pa 1976). 1999. PMID: 10065516
-
Biomechanical comparison of the stable efficacy of two anterior plating systems.Clin Biomech (Bristol). 2003 Jul;18(6):S59-66. doi: 10.1016/s0268-0033(03)00086-x. Clin Biomech (Bristol). 2003. PMID: 12828916
-
Anterior cervical fixation: analysis of load-sharing and stability with use of static and dynamic plates.J Bone Joint Surg Am. 2006 Jul;88(7):1566-73. doi: 10.2106/JBJS.E.00305. J Bone Joint Surg Am. 2006. PMID: 16818983 Clinical Trial.
-
Comparison of allograft to autograft in multilevel anterior cervical discectomy and fusion with rigid plate fixation.Spine J. 2003 Nov-Dec;3(6):451-9. doi: 10.1016/s1529-9430(03)00173-6. Spine J. 2003. PMID: 14609689
-
[Ventral interbody spondylodesis in injuries of the cervical spine. Indications, surgical technique and results].Zentralbl Chir. 1998;123(8):919-29. Zentralbl Chir. 1998. PMID: 9757537 Review. German.
Cited by
-
A unique modular implant system enhances load sharing in anterior cervical interbody fusion: a finite element study.Biomed Eng Online. 2014 Mar 11;13(1):26. doi: 10.1186/1475-925X-13-26. Biomed Eng Online. 2014. PMID: 24618205 Free PMC article.
References
-
- Balabhadra RS, Kim DH, Zhang HY. Anterior cervical fusion using dense cancellous allografts and dynamic plating. Neurosurgery. 2004;54:1405–1141. discussion 1411-1402. - PubMed
-
- Bolesta MJ, Rechtine GR, 2nd, Chrin AM. One- and two-level anterior cervical discectomy and fusion: the effect of plate fixation. Spine J. 2002;2:197–203. - PubMed
-
- Brodke DS, Gollogly S, Alexander Mohr R, Nguyen BK, Dailey AT, Bachus aK. Dynamic cervical plates: biomechanical evaluation of load sharing and stiffness. Spine. 2001;26:1324–1329. - PubMed
-
- Brodke DS, Klimo P, Jr, Bachus KN, Braun JT, Dailey AT. Anterior cervical fixation : analysis of load-sharing and stability with use of static and dynamic plates. J Bone Joint Surg Am. 2006;88:1566–1573. - PubMed
-
- Caspar W, Geisler FH, Pitzen T, Johnson TA. Anterior cervical plate stabilization in one- and two-level degenerative disease: overtreatment or benefit? J Spinal Disord. 1998;11:1–11. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
