

Children with orofacial clefts: health-care use and costs among a privately insured population
- PMID: 19445422
- PMCID: PMC2663882
- DOI: 10.1177/003335490912400315
Children with orofacial clefts: health-care use and costs among a privately insured population
Abstract
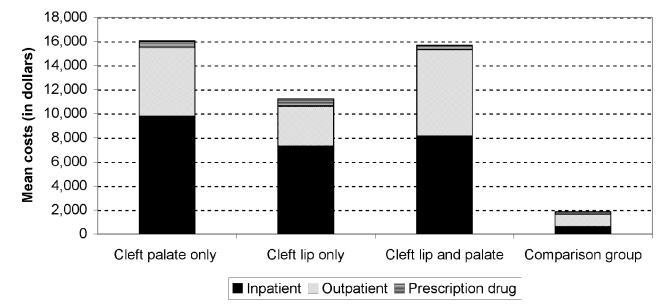
Objectives: Orofacial clefts are common birth defects that often require multiple surgeries and medical treatments during childhood. We used healthcare insurance claims data to estimate health-care expenditures for infants and children < or = 10 years of age with an orofacial cleft.
Methods: The data were derived from the 2000-2004 MarketScan Commercial Claims and Encounters databases, which include person-specific information on health-care use, expenditures, and enrollment for approximately 50 large employers, health plans, and government and public organizations. Health insurance claims data from 821,619 children < or = 10 years of age enrolled in employer-sponsored plans during 2004 were analyzed. Expenditures for inpatient admissions, outpatient services, and prescription drug claims were calculated for children with and those without an orofacial cleft.
Results: The difference in annual mean costs (i.e., incremental costs) between children aged 0 through 10 years with an orofacial cleft and those without an orofacial cleft was $13,405. The mean and median costs for children < or = 10 years of age with an orofacial cleft were eight times higher than for children of the same age without an orofacial cleft. Mean costs for infants with a cleft and another major, unrelated defect were 25 times higher than those for an infant without a cleft, and five times higher than for infants with an isolated cleft.
Conclusion: These findings document substantially elevated medical care costs for privately insured children with an orofacial cleft. Additional study of the economic burden associated with this condition should include a broader range of economic costs.
Figures
References
-
- Arosarena OA. Cleft lip and palate. Otolaryngol Clin North Am. 2007;40:27–60. - PubMed
-
- Canfield MA, Honein MA, Yuskiv N, Xing J, Mai CT, Collins JS, et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999–2001. Birth Defects Res A Clin Mol Teratol. 2006;76:747–56. - PubMed
-
- Bender PL. Genetics of cleft lip and palate. J Pediatr Nurs. 2000;15:242–9. - PubMed
-
- Ngai CW, Martin WL, Tonks A, Wyldes MP, Kilby MD. Are isolated facial cleft lip and palate associated with increased perinatal mortality? A cohort study from the West Midlands Region, 1995–1997. J Matern Fetal Neonatal Med. 2005;17:203–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
