

Treatment patterns for early pregnancy failure in Michigan
- PMID: 19445643
- PMCID: PMC2851131
- DOI: 10.1089/jwh.2008.1091
Treatment patterns for early pregnancy failure in Michigan
Abstract
Aims: We describe current treatment patterns for early pregnancy failure (EPF) among women enrolled in two Michigan health plans.
Methods: We conducted a retrospective review of EPF treatment among Michigan Medicaid enrollees between January 1, 2001, and December 31, 2004, and enrollees of a university-affiliated health plan between January 1, 2001, and December 31, 2005. Episodes were identified by the presence of a diagnostic code for EPF. Surgical treatment was distinguished from nonsurgical management using procedure codes. Facility charges, procedure, and place of service codes were used to determine whether a procedure was done in an office as opposed to an operating room. Cases without a claim for surgical uterine evacuation were examined for a misoprostol pharmacy claim and, if present, were classified as medical management. Cases without a procedure or pharmacy claim were classified as expectant management.
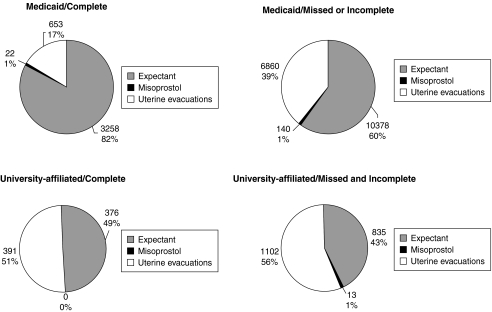
Results: Respectively, we identified 21,311 and 1,493 episodes of EPF in the Medicaid and university-affiliated health plan databases, respectively. Women enrolled in Medicaid were more likely to be treated with surgery than were enrollees of the university-affiliated health plan (35.3 vs. 18.0%, respectively, p < 0.000). Among Medicaid enrollees, only 0.5% of surgical evacuations occurred in the office, but office procedures were common among enrollees of the university-affiliated health plan (30.5%, p < 0.000). The proportion of cases managed with misoprostol was <1% in both groups. Caucasian race and age were both associated with having a surgical uterine evacuation (p < 0.001).
Conclusions: EPF is primarily being treated with expectant management or surgical evacuation in an operating room and may not reflect evidence-based practices or patient preferences.
Figures

References
-
- Rocconi RP. Chiang S. Richter HE. Straughn JM. Management strategies for abnormal early pregnancy: A cost-effectiveness analysis. J Reprod Med. 2005;50:486–490. - PubMed
-
- Blohm F. Friden B. Platz-Christensen JJ. Milsom I. Nielsen S. Expectant management of first-trimester miscarriage in clinical practice. Acta Obstet Gynecol Scand. 2003;82:654–658. - PubMed
-
- Nielsen S. Hahlin M. Expectant management of first-trimester spontaneous abortion. Lancet. 1995;345:84–86. - PubMed
-
- Chipchase J. James D. Randomised trial of expectant versus surgical management of spontaneous miscarriage. Br J Obstet Gynaecol. 1997;104:840–841. - PubMed
-
- Jurkovic D. Ross JA. Nicolaides KH. Expectant management of missed miscarriage. Br J Obstet Gynaecol. 1998;105:670–671. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
