

Impact of movement training on upper limb motor strategies in persons with shoulder impingement syndrome
- PMID: 19445724
- PMCID: PMC2694775
- DOI: 10.1186/1758-2555-1-8
Impact of movement training on upper limb motor strategies in persons with shoulder impingement syndrome
Abstract
Background: Movement deficits, such as changes in the magnitude of scapulohumeral and scapulathoracic muscle activations or perturbations in the kinematics of the glenohumeral, sternoclavicular and scapulothoracic joints, have been observed in people with shoulder impingement syndrome. Movement training has been suggested as a mean to contribute to the improvement of the motor performance in persons with musculoskeletal impairments. However, the impact of movement training on the movement deficits of persons with shoulder impingement syndrome is still unknown. The aim of this study was to evaluate the short-term effects of supervised movement training with feedback on the motor strategies of persons with shoulder impingement syndrome.
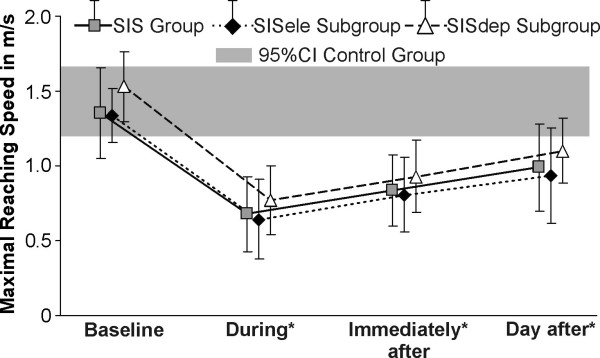
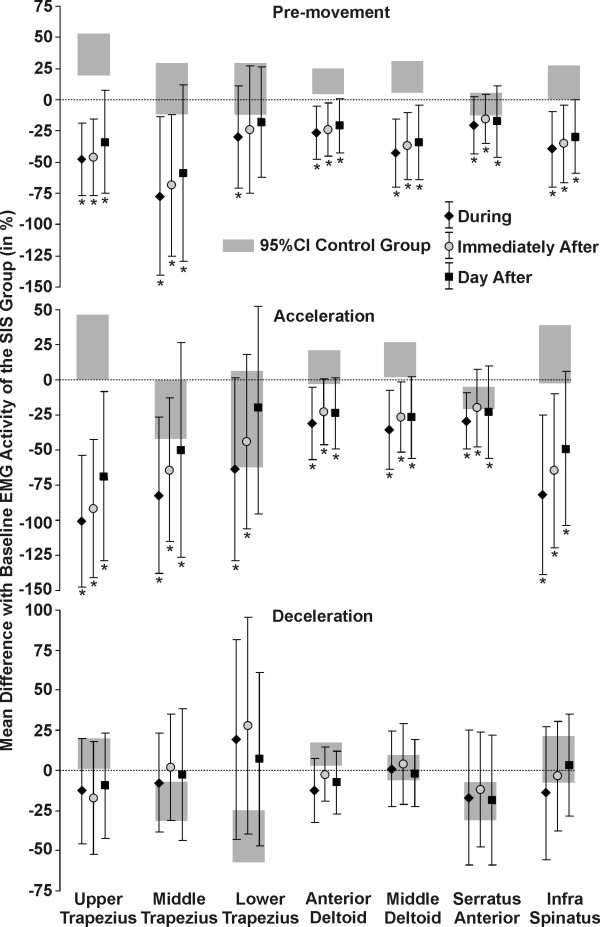
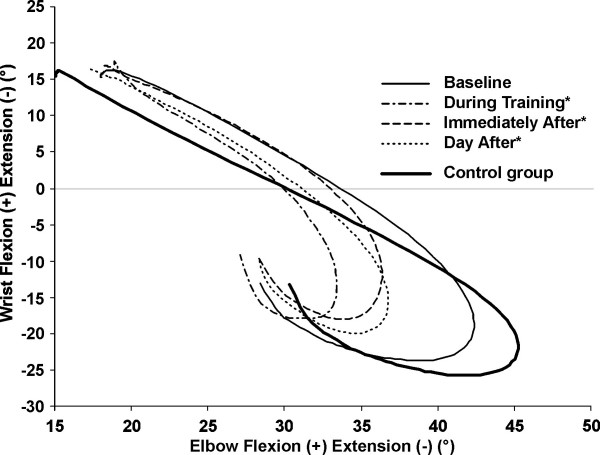
Methods: Thirty-three subjects with shoulder impingement were recruited. They were involved in two visits, one day apart. During the first visit, supervised movement training with feedback was performed. The upper limb motor strategies were evaluated before, during, immediately after and 24 hours after movement training. They were characterized during reaching movements in the frontal plane by EMG activity of seven shoulder muscles and total excursion and final position of the wrist, elbow, shoulder, clavicle and trunk. Movement training consisted of reaching movements performed under the supervision of a physiotherapist who gave feedback aimed at restoring shoulder movements. One-way repeated measures ANOVAs were run to analyze the effect of movement training.
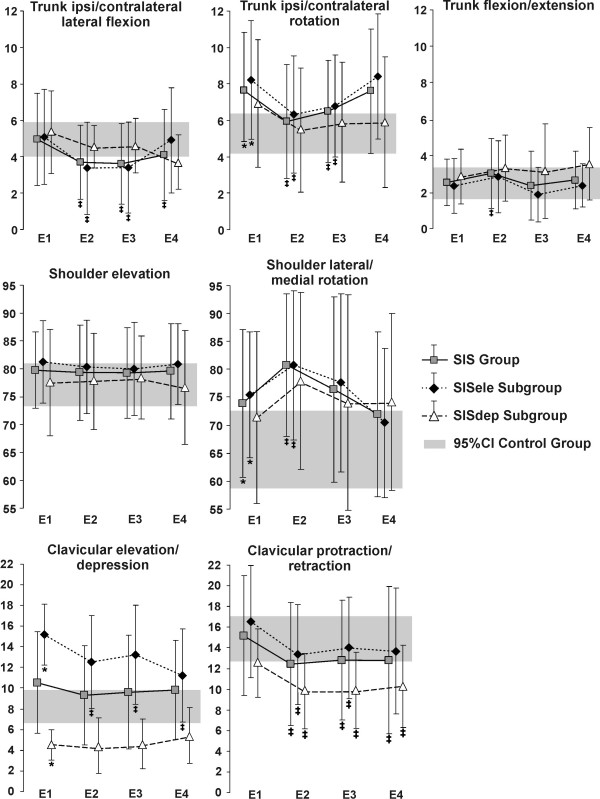
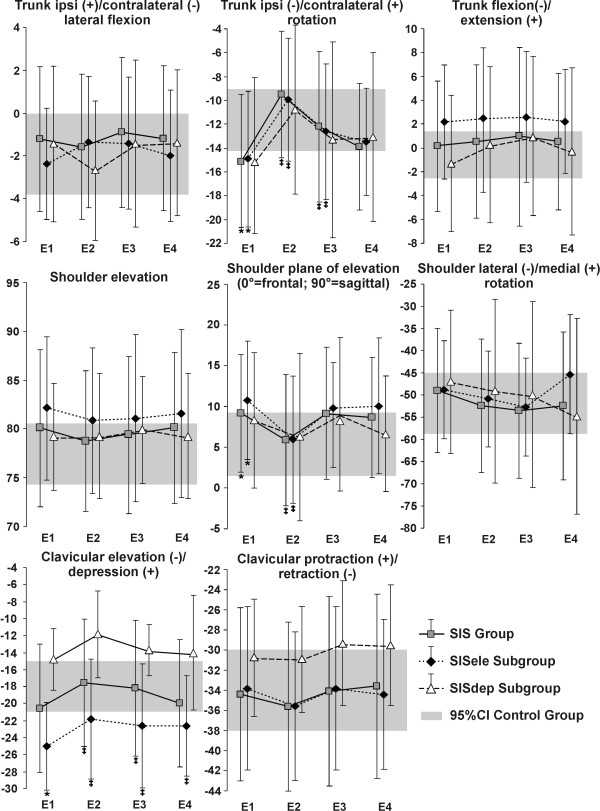
Results: During, immediately after and 24 hours after movement training with feedback, the EMG activity was significantly decreased compared to the baseline level. For the kinematics, total joint excursion of the trunk and final joint position of the trunk, shoulder and clavicle were significantly improved during and immediately after training compared to baseline. Twenty-four hours after supervised movement training, the kinematics of trunk, shoulder and clavicle were back to the baseline level.
Conclusion: Movement training with feedback brought changes in motor strategies and improved temporarily some aspects of the kinematics. However, one training session was not enough to bring permanent improvement in the kinematic patterns. These results demonstrate the potential of movement training in the rehabilitation of movement deficits associated with shoulder impingement syndrome.
Figures
References
LinkOut - more resources
Full Text Sources
