

Comparison of drug dosing recommendations based on measured GFR and kidney function estimating equations
- PMID: 19446939
- PMCID: PMC2756662
- DOI: 10.1053/j.ajkd.2009.03.008
Comparison of drug dosing recommendations based on measured GFR and kidney function estimating equations
Abstract
Background: Kidney disease alters the pharmacokinetic disposition of many medications, requiring dosage adjustment to maintain therapeutic serum concentrations. The Cockcroft-Gault (CG) equation is used for pharmacokinetic studies and drug dosage adjustments, but the Modification of Diet in Renal Disease (MDRD) Study equation is more accurate and more often reported by clinical laboratories than the CG equation.
Study design: Diagnostic test study.
Settings & participants: Pooled data set for 5,504 participants from 6 research studies and 4 clinical populations with measured glomerular filtration rate (GFR).
Index test: Estimated kidney function using the MDRD Study and CG equations incorporating actual (CG) or ideal body weight (CG(IBW)) and standardized serum creatinine concentrations.
Reference test: Measured GFR assessed by using iodine-125-iothalamate urinary clearance.
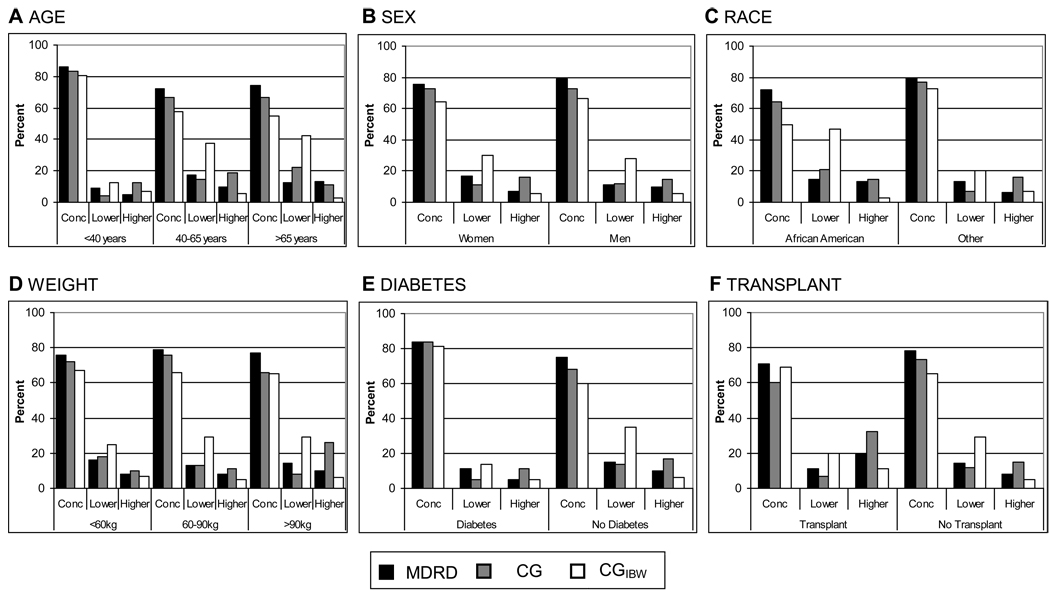
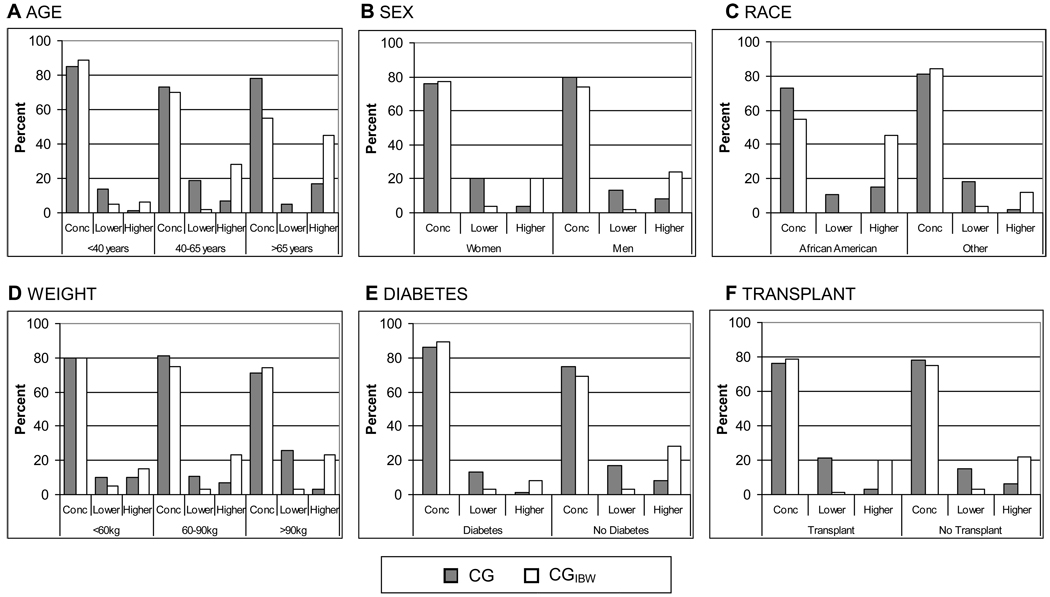
Outcome: Concordance of assigned kidney function categories designated by the Food and Drug Administration (FDA) Guidance for Industry for pharmacokinetic studies and recommended dosages of 15 medications cleared by the kidneys.
Results: Concordance of kidney function estimates with measured GFR for FDA-assigned kidney function categories was 78% for the MDRD Study equation compared with 73% for the CG equation (P < 0.001) and 66% for the CG(IBW) equation (P < 0.001). Concordance between the MDRD Study equation and CG and CG(IBW) equations was 78% and 75%, respectively (P < 0.001). Concordance of kidney function estimates with measured GFR for recommended drug dosages was 88% for MDRD Study equation compared with 85% for the CG equation (P < 0.001) and 82% for the CG(IBW) equation (P < 0.001), with lower concordance when dosing recommendations for drugs included narrow GFR ranges. Concordance rates between the CG and CG(IBW) equations and MDRD Study equation were 89% and 88%, respectively (P < 0.05).
Limitations: Results based on simulation rather than pharmacokinetic studies. Outcome was drug dosage recommendations, rather than observed drug efficacy and safety.
Conclusions: The MDRD Study equation can also be used for pharmacokinetic studies and drug dosage adjustments. As more accurate GFR-estimating equations are developed, they should be used for these purposes.
Figures
Comment in
-
Estimated GFR for drug dosing: a bedside formula.Am J Kidney Dis. 2009 Nov;54(5):982-3; author reply 985-6. doi: 10.1053/j.ajkd.2009.07.027. Am J Kidney Dis. 2009. PMID: 19853205 No abstract available.
-
Drug dose adjustments in patients with renal impairment.Am J Kidney Dis. 2009 Nov;54(5):983-4; author reply 985-6. doi: 10.1053/j.ajkd.2009.07.025. Am J Kidney Dis. 2009. PMID: 19853206 No abstract available.
-
Estimated GFR vs creatinine clearance for drug dosing.Am J Kidney Dis. 2009 Nov;54(5):984-5; author reply 985-6. doi: 10.1053/j.ajkd.2009.08.015. Am J Kidney Dis. 2009. PMID: 19853207 No abstract available.
-
Use of the MDRD study equation for drug dosing.Am J Kidney Dis. 2009 Nov;54(5):984; author reply 985-6. doi: 10.1053/j.ajkd.2009.07.026. Am J Kidney Dis. 2009. PMID: 19853208 No abstract available.
References
-
- Food and Drug Administration. Guidance for Industry: Pharmacokinetics in Patients with Impaired Renal Function — Study Design, Data Analysis, and Impact on Dosing and Labeling. Rockville: U.S. Department of Health and Human Services; 1998. May,
-
- Stevens LA, Manzi J, Levey AS, et al. Impact of creatinine calibration on performance of GFR estimating equations in a pooled individual patient database. Am J Kidney Dis. 2007;50(1):21–35. - PubMed
-
- Coresh J, Stevens LA. Kidney function estimating equations: Where do we stand? Curr Opin Nephrol Hypertens. 2006;15(3):276–284. - PubMed
-
- Lewis JB, Agodoa L, Cheek D, et al. Comparison of cross-sectional renal function measurements in African-Americans with hypertensive nephrosclerosis and of primary formulas to estimate glomerular filtration rate. Am J Kidney Dis. 2001 Oct;38(4):744–753. - PubMed
-
- Froissart M, Rossert J, Jacquot C, Paillard M, Houillier P. Predictive performance of the modification of diet in renal disease and Cockcroft-Gault equations for estimating renal function. J Am Soc Nephrol. 2005 Mar;16(3):763–773. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
