

Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection
- PMID: 19447923
- PMCID: PMC2821291
- DOI: 10.1378/chest.08-1190
Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection
Abstract
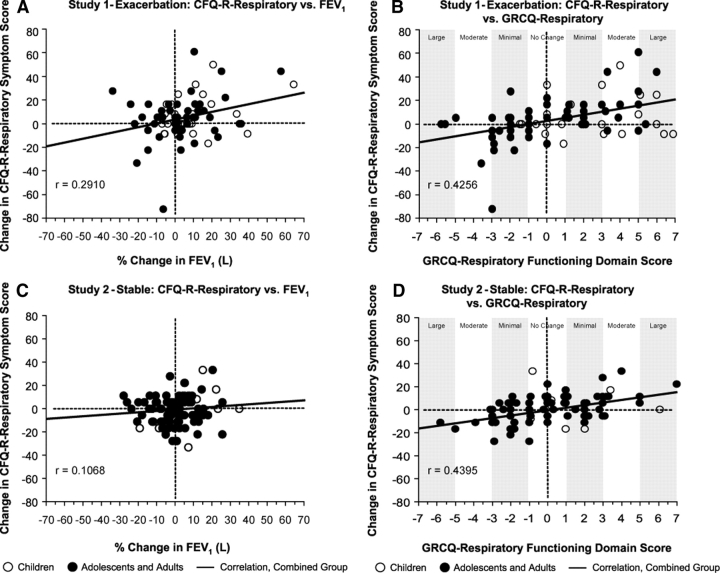
Background: The Cystic Fibrosis Questionnaire-Revised (CFQ-R) is a validated patient-reported outcome (PRO) containing both generic scales and scales specific to cystic fibrosis (CF). The minimal clinically important difference (MCID) score for a PRO corresponds to the smallest clinically relevant change a patient can detect. MCID scores for the CFQ-R respiratory symptom (CFQ-R-Respiratory) scale were determined using data from two 28 day, open-label, tobramycin inhalation solution (TIS) studies in patients with CF and chronic Pseudomonas aeruginosa airway infection. At study enrollment, patients in the study 1-exacerbation had symptoms indicative of pulmonary exacerbation (n = 84; < 14 years of age, 31 patients; > or = 14 years of age, 53 patients); patients in study 2-stable had stable respiratory symptoms (n = 140; < 14 years of age, 14 patients; > or = 14 years, 126 patients).
Methods: The anchor-based method utilized a global rating-of-change questionnaire (GRCQ) that assessed patients' perceptions of change in their respiratory symptoms after TIS treatment. The mean change from baseline CFQ-R-Respiratory scores were mapped onto the GRCQ to estimate the MCID. The two distribution-based methods were as follows: (1) 0.5 SD of mean change in CFQ-R-Respiratory scores (baseline to end of TIS treatment); and (2) 1 SEM for baseline CFQ-R-Respiratory scores. Triangulation of these three estimates defined the MCIDs.
Results: MCID scores were larger for patients in study 1-exacerbation (8.5 points) than for those in study 2-stable (4.0 points), likely reflecting differences in patient disease status (exacerbation/stable) between these studies.
Conclusions: Patient benefit from new and current CF therapies can be evaluated using changes in CFQ-R-Respiratory scores. Using the MCID provides a systematic way to interpret these changes, and facilitates the identification of CF treatments that improve both symptoms and physiologic variables, potentially leading to better treatment adherence and clinical outcomes. Trial registration (study 1-exacerbation): Australian-New Zealand Clinical Trials Registry Identifier: ACTRN 12605000602628 Trial registration (study 2-stable): ClinicalTrials.gov Identifier: NCT00104520.
Figures
References
-
- Turner RR, Quittner AL, Parasuraman BM, et al. Patient-reported outcomes: instrument development and selection issues. Value Health. 2007;10(suppl):S86–S93. - PubMed
-
- Abbott J, Gee L. Quality of life in children and adolescents with cystic fibrosis: implications for optimizing treatments and clinical trial design. Pediatr Drugs. 2005;5:41–56. - PubMed
-
- Terwee CB, Dekker FW, Wiersinga WM, et al. On assessing responsiveness of health-related quality of life instruments: guidelines for instrument evaluation. Qual Life Res. 2003;12:349–362. - PubMed
-
- Guyatt GH. Making sense of quality-of-life data. Med Care. 2000;38:175–179. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- M01 RR000400/RR/NCRR NIH HHS/United States
- M01 RR00065/RR/NCRR NIH HHS/United States
- M01 RR000034/RR/NCRR NIH HHS/United States
- M01 RR000082/RR/NCRR NIH HHS/United States
- R01 FD003016/FD/FDA HHS/United States
- M01 RR00400/RR/NCRR NIH HHS/United States
- M01 RR000065/RR/NCRR NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- M01 RR10710/RR/NCRR NIH HHS/United States
- M01 RR00037/RR/NCRR NIH HHS/United States
- M01 RR00070/RR/NCRR NIH HHS/United States
- M01 RR00039/RR/NCRR NIH HHS/United States
- M01 RR000046/RR/NCRR NIH HHS/United States
- M01 RR00188/RR/NCRR NIH HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- M01 RR01066/RR/NCRR NIH HHS/United States
- M01 RR002172/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000037/RR/NCRR NIH HHS/United States
- M01 RR00827/RR/NCRR NIH HHS/United States
- M01 RR00046/RR/NCRR NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- M01 RR000489/RR/NCRR NIH HHS/United States
- M01 RR00043/RR/NCRR NIH HHS/United States
- M01 RR010710/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- M01 RR00750/RR/NCRR NIH HHS/United States
- M01 RR023940/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- M01 RR00069/RR/NCRR NIH HHS/United States
- M01 RR00064/RR/NCRR NIH HHS/United States
- M01 RR00042/RR/NCRR NIH HHS/United States
- M01 RR02172/RR/NCRR NIH HHS/United States
- M01 RR10733/RR/NCRR NIH HHS/United States
- M01 RR000042/RR/NCRR NIH HHS/United States
- M01 RR00034/RR/NCRR NIH HHS/United States
- M01 RR001070/RR/NCRR NIH HHS/United States
- M01 RR00082/RR/NCRR NIH HHS/United States
- M01 RR000064/RR/NCRR NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
