

Reduced EGFR causes abnormal valvular differentiation leading to calcific aortic stenosis and left ventricular hypertrophy in C57BL/6J but not 129S1/SvImJ mice
- PMID: 19448146
- PMCID: PMC2711734
- DOI: 10.1152/ajpheart.00866.2008
Reduced EGFR causes abnormal valvular differentiation leading to calcific aortic stenosis and left ventricular hypertrophy in C57BL/6J but not 129S1/SvImJ mice
Abstract
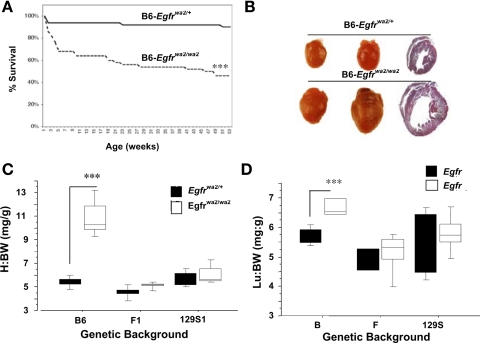
Epidermal growth factor receptor (EGFR) signaling contributes to aortic valve development in mice. Because developmental phenotypes in Egfr-null mice are dependent on genetic background, the hypomorphic Egfr(wa2) allele was made congenic on C57BL/6J (B6) and 129S1/SvImJ (129) backgrounds and used to identify the underlying cellular cause of EGFR-related aortic valve abnormalities. Egfr(wa2/wa2) mice on both genetic backgrounds develop aortic valve hyperplasia. Many B6-Egfr(wa2/wa2) mice die before weaning, and those surviving to 3 mo of age or older develop severe left ventricular hypertrophy and heart failure. The cardiac phenotype was accompanied by significantly thicker aortic cusps and larger transvalvular gradients in B6-Egfr(wa2/wa2) mice compared with heterozygous controls and age-matched Egfr(wa2) homozygous mice on either 129 or B6129F1 backgrounds. Histological analysis revealed cellular changes in B6-Egfr(wa2/wa2) aortic valves underlying elevated pressure gradients and progression to heart failure, including increased cellular proliferation, ectopic cartilage formation, extensive calcification, and inflammatory infiltrate, mimicking changes seen in human calcific aortic stenosis. Despite having congenitally enlarged valves, 129 and B6129F1-Egfr(wa2/wa2) mice have normal lifespans, absence of left ventricular hypertrophy, and normal systolic function. These results show the requirement of EGFR activity for normal valvulogenesis and demonstrate that dominantly acting genetic modifiers curtail pathological changes in congenitally deformed valves. These studies provide a novel model of aortic sclerosis and stenosis and suggest that long-term inhibition of EGFR signaling for cancer therapy may have unexpected consequences on aortic valves in susceptible individuals.
Figures





Similar articles
-
Discovery of an Experimental Model of Unicuspid Aortic Valve.J Am Heart Assoc. 2018 Jun 30;7(13):e006908. doi: 10.1161/JAHA.117.006908. J Am Heart Assoc. 2018. PMID: 29960994 Free PMC article.
-
Cardiac response to pressure overload in 129S1/SvImJ and C57BL/6J mice: temporal- and background-dependent development of concentric left ventricular hypertrophy.Am J Physiol Heart Circ Physiol. 2007 May;292(5):H2119-30. doi: 10.1152/ajpheart.00816.2006. Epub 2006 Dec 15. Am J Physiol Heart Circ Physiol. 2007. PMID: 17172276
-
Early development of calcific aortic valve disease and left ventricular hypertrophy in a mouse model of combined dyslipidemia and type 2 diabetes mellitus.Arterioscler Thromb Vasc Biol. 2014 Oct;34(10):2283-91. doi: 10.1161/ATVBAHA.114.304205. Epub 2014 Aug 14. Arterioscler Thromb Vasc Biol. 2014. PMID: 25231636
-
Calcific Aortic Valve Disease: Part 2-Morphomechanical Abnormalities, Gene Reexpression, and Gender Effects on Ventricular Hypertrophy and Its Reversibility.J Cardiovasc Transl Res. 2016 Aug;9(4):374-99. doi: 10.1007/s12265-016-9695-z. Epub 2016 May 16. J Cardiovasc Transl Res. 2016. PMID: 27184804 Free PMC article. Review.
-
Sex-Specific Features of Calcific Aortic Valve Disease.Int J Mol Sci. 2020 Aug 6;21(16):5620. doi: 10.3390/ijms21165620. Int J Mol Sci. 2020. PMID: 32781508 Free PMC article. Review.
Cited by
-
Multi-Omics Approaches to Define Calcific Aortic Valve Disease Pathogenesis.Circ Res. 2021 Apr 30;128(9):1371-1397. doi: 10.1161/CIRCRESAHA.120.317979. Epub 2021 Apr 29. Circ Res. 2021. PMID: 33914608 Free PMC article. Review.
-
Cardiac teratogenicity in mouse maternal phenylketonuria: defining phenotype parameters and genetic background influences.Mol Genet Metab. 2012 Dec;107(4):650-8. doi: 10.1016/j.ymgme.2012.08.001. Epub 2012 Aug 8. Mol Genet Metab. 2012. PMID: 22951387 Free PMC article.
-
Aortic regurgitation and heart valve disease in mice.J Thorac Dis. 2015 Oct;7(10):1676-7. doi: 10.3978/j.issn.2072-1439.2015.10.14. J Thorac Dis. 2015. PMID: 26623080 Free PMC article. No abstract available.
-
Shear Stress Induces a Time-Dependent Inflammatory Response in Human Monocyte-Derived Macrophages.Ann Biomed Eng. 2024 Nov;52(11):2932-2947. doi: 10.1007/s10439-024-03546-5. Epub 2024 Sep 17. Ann Biomed Eng. 2024. PMID: 39289258
-
Galnt1 is required for normal heart valve development and cardiac function.PLoS One. 2015 Jan 23;10(1):e0115861. doi: 10.1371/journal.pone.0115861. eCollection 2015. PLoS One. 2015. PMID: 25615642 Free PMC article.
References
-
- Alipour MS, Shah PA. Diagnosis of aortic stenosis in the elderly: role of echocardiography. Am J Geriatr Cardiol 12: 201–206, 2003. - PubMed
-
- Barrick CJ, Rojas M, Schoonhoven R, Smyth SS, Threadgill DW. Cardiac response to pressure overload in 129S1/SvImJ and C57BL/6J mice: temporal- and background-dependent development of concentric left ventricular hypertrophy. Am J Physiol Heart Circ Physiol 292: H2119–H2130, 2007. - PubMed
-
- Bonow RO, Carabello B, de Leon AC Jr, Edmunds LH Jr, Fedderly BJ, Freed MD, Gaasch WH, McKay CR, Nishimura RA, O'Gara PT, O'Rourke RA, Rahimtoola SH, Ritchie JL, Cheitlin MD, Eagle KA, Gardner TJ, Garson A Jr, Gibbons RJ, Russell RO, Ryan TJ, Smith SC Jr. Guidelines for the management of patients with valvular heart disease: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). Circulation 98: 1949–1984, 1998. - PubMed
-
- Bonow RO, Carabello BA, Kanu C, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 114: e84–e231, 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous