

Distal potassium handling based on flow modulation of maxi-K channel activity
- PMID: 19448535
- PMCID: PMC3151167
- DOI: 10.1097/MNH.0b013e32832c75d8
Distal potassium handling based on flow modulation of maxi-K channel activity
Abstract
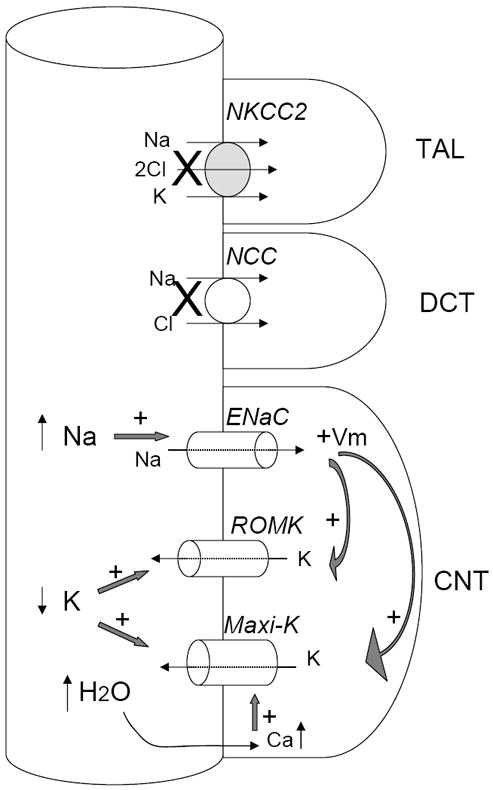
Purpose of review: Studies on the mechanisms of distal K+ secretion have highlighted the importance of the renal outer-medullary K+ (ROMK) and maxi-K channels. This review considers several human disorders characterized by hypokalemia and hyperkalemia, as well as mouse models of these disorders, and the mechanisms by which ROMK and maxi-K may be dysregulated.
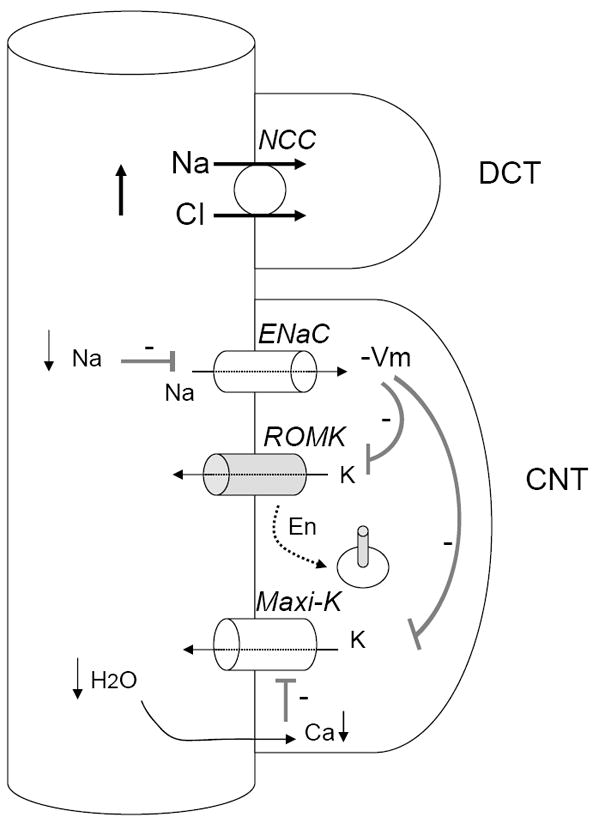
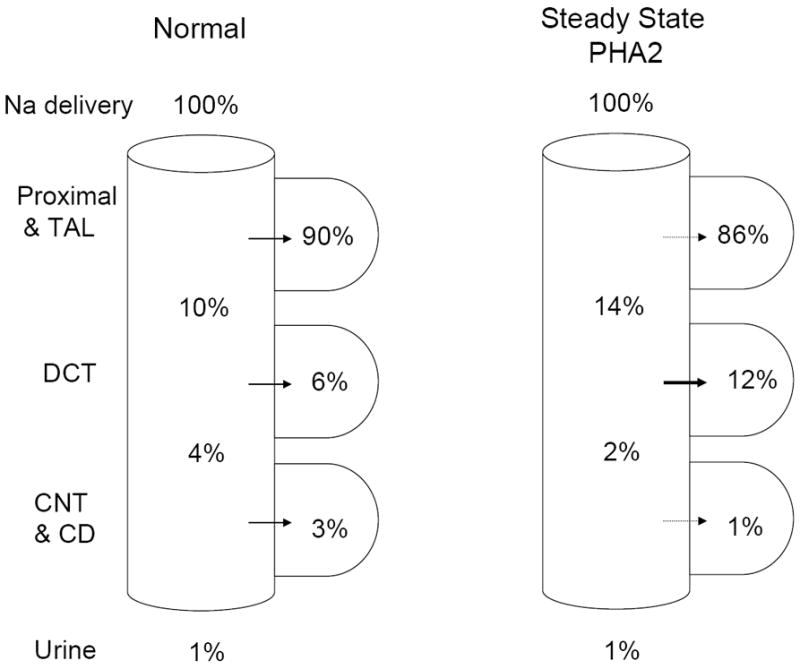
Recent findings: Analysis of knockout mice lacking ROMK, a model for type II Bartter's syndrome, has shown a role for maxi-K in distal K+ secretion. Knockout mice lacking either the alpha or beta1 subunits of maxi-K also show deficits in flow-dependent K+ secretion. Analysis of transgenic and knock-in mouse models of pseudohypoaldosteronism type II, in which mutant forms of with-no-lysine kinase 4 are expressed, suggests ways in which ROMK and maxi-K may be dysregulated to result in hyperkalemia. Modeling studies also provide insights into the role of Na+ delivery vs. flow in K+ secretion.
Summary: The importance of both ROMK and maxi-K to distal K+ secretion is now well established, but the relative role that each of these two channels plays in normal and diseased states has not been definitively established. Analysis of human and animal model data can generate hypotheses for future experiments.
Figures
References
-
- Malnic G, Klose RM, Giebisch G. Micropuncture study of renal potassium excretion in the rat. Am J Physiol. 1964;206:674–686. - PubMed
-
- Hebert SC. An ATP-regulated, inwardly rectifying potassium channel from rat kidney (ROMK) Kidney Int. 1995;48:1010–1016. - PubMed
-
- Pluznick JL, Sansom SC. BK channels in the kidney: role in K+ secretion and localization of molecular components. Am J Physiol Renal Physiol. 2006;291:F517–F529. - PubMed
-
- Meneton P, Loffing J, Warnock DG. Sodium and potassium handling by the aldosterone-sensitive distal nephron: the pivotal role of the distal and connecting tubule. Am J Physiol Renal Physiol. 2004;287:F593–F601. - PubMed
-
- Palmer LG, Frindt G. Na+ and K+ transport by the renal connecting tubule. Curr Opin Nephrol Hypertens. 2007;16:477–483. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
