

Impaired interferon signaling is a common immune defect in human cancer
- PMID: 19451644
- PMCID: PMC2690021
- DOI: 10.1073/pnas.0901329106
Impaired interferon signaling is a common immune defect in human cancer
Abstract
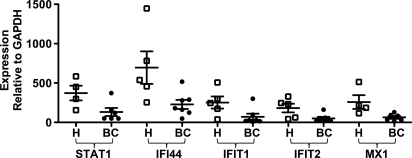
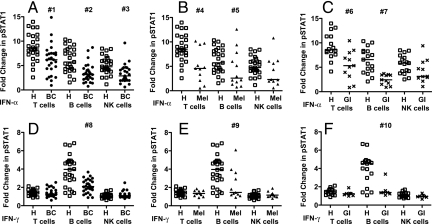
Immune dysfunction develops in patients with many cancer types and may contribute to tumor progression and failure of immunotherapy. Mechanisms underlying cancer-associated immune dysfunction are not fully understood. Efficient IFN signaling is critical to lymphocyte function; animals rendered deficient in IFN signaling develop cancer at higher rates. We hypothesized that altered IFN signaling may be a key mechanism of immune dysfunction common to cancer. To address this, we assessed the functional responses to IFN in peripheral blood lymphocytes from patients with 3 major cancers: breast cancer, melanoma, and gastrointestinal cancer. Type-I IFN (IFN-alpha)-induced signaling was reduced in T cells and B cells from all 3 cancer-patient groups compared to healthy controls. Type-II IFN (IFN-gamma)-induced signaling was reduced in B cells from all 3 cancer patient groups, but not in T cells or natural killer cells. Impaired-IFN signaling was equally evident in stage II, III, and IV breast cancer patients, and downstream functional defects in T cell activation were identified. Taken together, these findings indicate that defects in lymphocyte IFN signaling arise in patients with breast cancer, melanoma, and gastrointestinal cancer, and these defects may represent a common cancer-associated mechanism of immune dysfunction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Down-regulation of the interferon signaling pathway in T lymphocytes from patients with metastatic melanoma.PLoS Med. 2007 May;4(5):e176. doi: 10.1371/journal.pmed.0040176. PLoS Med. 2007. PMID: 17488182 Free PMC article.
-
Angiogenic and immune parameters during recombinant interferon-alpha2b adjuvant treatment in patients with melanoma.Oncol Res. 2000;12(5):241-51. doi: 10.3727/096504001108747738. Oncol Res. 2000. PMID: 11417749 Clinical Trial.
-
Impact of Interferon-alpha1b (IFN-α1b) on Antitumor Immune Response: An Interpretation of the Promising Therapeutic Effect of IFN-alpha1b on Melanoma.Med Sci Monit. 2020 Mar 14;26:e922790. doi: 10.12659/MSM.922790. Med Sci Monit. 2020. PMID: 32210221 Free PMC article.
-
Immunologically-mediated tumour cell apoptosis: the role of TRAIL in T cell and cytokine-mediated responses to melanoma.Forum (Genova). 2000 Jul-Sep;10(3):243-52. Forum (Genova). 2000. PMID: 11007932 Review.
-
[Interferon gamma as a regulator of immune cell function].Postepy Hig Med Dosw. 1999;53(1):23-41. Postepy Hig Med Dosw. 1999. PMID: 10352545 Review. Polish.
Cited by
-
The duality of STAT2 mediated type I interferon signaling in the tumor microenvironment and chemoresistance.Cytokine. 2023 Jan;161:156081. doi: 10.1016/j.cyto.2022.156081. Epub 2022 Oct 31. Cytokine. 2023. PMID: 36327541 Free PMC article. Review.
-
Expression profiles of human interferon-alpha and interferon-lambda subtypes are ligand- and cell-dependent.Immunol Cell Biol. 2012 Sep;90(8):774-83. doi: 10.1038/icb.2011.109. Epub 2012 Jan 17. Immunol Cell Biol. 2012. PMID: 22249201 Free PMC article.
-
PKR induces TGF-β and limits oncolytic immune therapy.J Immunother Cancer. 2023 Feb;11(2):e006164. doi: 10.1136/jitc-2022-006164. J Immunother Cancer. 2023. PMID: 36796878 Free PMC article.
-
Polymorphism of IFN-γ +874T/A associated with production of IFN-γ affects human papillomavirus susceptibility in rural women from Luohe, Henan, China.Onco Targets Ther. 2018 Jul 25;11:4339-4344. doi: 10.2147/OTT.S161544. eCollection 2018. Onco Targets Ther. 2018. PMID: 30100739 Free PMC article.
-
Characterization of osteosarcoma subtypes mediated by macrophage-related genes and creation and validation of a risk score system to quantitatively assess the prognosis of osteosarcoma and reflect the tumor microenvironment.Ann Transl Med. 2022 Dec;10(24):1318. doi: 10.21037/atm-22-5613. Ann Transl Med. 2022. PMID: 36660647 Free PMC article.
References
-
- Lee PP, et al. Characterization of circulating T cells specific for tumor-associated antigens in melanoma patients. Nat Med. 1999;5:677–685. - PubMed
-
- Anichini A, et al. An expanded peripheral T cell population to a cytotoxic T lymphocyte (CTL)-defined, melanocyte-specific antigen in metastatic melanoma patients impacts on generation of peptide-specific CTLs but does not overcome tumor escape from immune surveillance in metastatic lesions. J Exp Med. 1999;190:651–667. - PMC - PubMed
-
- Lee KH, et al. Increased vaccine-specific T cell frequency after peptide-based vaccination correlates with increased susceptibility to in vitro stimulation but does not lead to tumor regression. J Immunol. 1999;163:6292–6300. - PubMed
-
- Weber J, et al. Granulocyte-macrophage-colony-stimulating factor added to a multipeptide vaccine for resected stage II melanoma. Cancer. 2003;97:186–200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
