

Use of leukoreduced blood does not reduce infection, organ failure, or mortality following trauma
- PMID: 19452207
- PMCID: PMC7101844
- DOI: 10.1007/s00268-009-0076-5
Use of leukoreduced blood does not reduce infection, organ failure, or mortality following trauma
Abstract
Background: Leukoreduced (LR) blood has been demonstrated to reduce morbidity and mortality in high-risk surgical patients, but not in trauma patients. The objective of the present study was to determine the effect of LR blood on morbidity and mortality. We hypothesized that the use of LR blood does not improve outcome in trauma patients.
Methods: This study was a retrospective cohort analysis of trauma patients transfused at a level 1 Trauma Center from 2001 to 2004. Between 2002 and 2003, LR blood was transfused. Prior to that time and subsequent to it, non-leukoreduced (NLR) blood was transfused. This created two historical comparison groups. Data collected included patient demographics, units of blood transfused, intensive care unit (ICU) and hospital days, ventilator days, injury severity score (ISS), mortality, presence of acute respiratory distress syndrome (ARDS), and infectious complications. A multiple organ dysfunction syndrome (MODS) score was calculated.
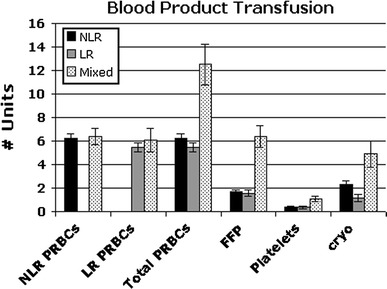
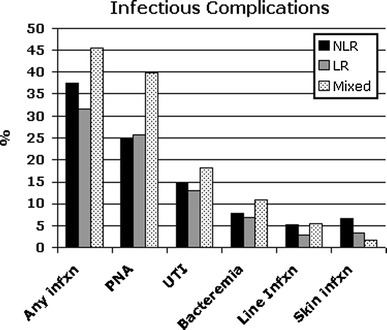
Results: The distribution of patients was as follows: 284 patients received only NLR blood, 153 received only LR blood, and 58 received at least one unit of each. The mean ISS was similar (NLR: 26, LR: 24; P > 0.1). No differences were seen between groups in units transfused (6.2 vs. 5.5), number of ICU days (8.2 vs. 9.0), number of hospital days (16.9 vs. 18.6), number of ventilator days (6.1 vs. 5.7), incidence of ARDS (8.3% vs. 8.5%), MODS score (5.5 vs. 5.9), mortality rate (15.1% vs. 15.7%), or infection rate (36% vs. 30%) (P > 0.1).
Conclusions: This study represents the largest series comparing trauma patients who received either LR or standard blood transfusions. The use of LR blood does not improve outcome in trauma patients.
Figures
Similar articles
-
Multiple organ failure in trauma patients.J Trauma. 2003 Oct;55(4):608-16. doi: 10.1097/01.TA.0000092378.10660.D1. J Trauma. 2003. PMID: 14566110
-
Prestorage leukoreduction ameliorates the effects of aging on banked blood.J Trauma. 2010 Aug;69(2):330-7. doi: 10.1097/TA.0b013e3181e0b253. J Trauma. 2010. PMID: 20699741 Free PMC article.
-
Allogenic blood transfusion in the first 24 hours after trauma is associated with increased systemic inflammatory response syndrome (SIRS) and death.Surg Infect (Larchmt). 2004 Winter;5(4):395-404. doi: 10.1089/sur.2004.5.395. Surg Infect (Larchmt). 2004. PMID: 15744131
-
Leukoreduction before red blood cell transfusion has no impact on mortality in trauma patients.J Surg Res. 2007 Mar;138(1):32-6. doi: 10.1016/j.jss.2006.07.048. Epub 2006 Dec 11. J Surg Res. 2007. PMID: 17161430
-
[Hemoglobin-oriented and coagulation factor-based algorithm : Effect on transfusion needs and standardized mortality rate in massively transfused trauma patients].Anaesthesist. 2015 Nov;64(11):828-38. doi: 10.1007/s00101-015-0093-8. Epub 2015 Oct 9. Anaesthesist. 2015. PMID: 26453580 Review. German.
Cited by
-
Risk factors for trauma-induced coagulopathy- and transfusion-associated multiple organ failure in severely injured trauma patients.Front Med (Lausanne). 2015 Apr 24;2:24. doi: 10.3389/fmed.2015.00024. eCollection 2015. Front Med (Lausanne). 2015. PMID: 25964951 Free PMC article.
-
Predictors of pulmonary failure following severe trauma: a trauma registry-based analysis.Scand J Trauma Resusc Emerg Med. 2013 Apr 22;21:34. doi: 10.1186/1757-7241-21-34. Scand J Trauma Resusc Emerg Med. 2013. PMID: 23607528 Free PMC article.
-
Impact of stored red cells on clinical outcome in critically ill.Asian J Transfus Sci. 2019 Jan-Jun;13(1):17-22. doi: 10.4103/ajts.AJTS_76_18. Asian J Transfus Sci. 2019. PMID: 31360005 Free PMC article.
-
Resuscitation with washed aged packed red blood cell units decreases the proinflammatory response in mice after hemorrhage.J Trauma Acute Care Surg. 2012 Aug;73(2 Suppl 1):S128-33. doi: 10.1097/TA.0b013e3182606301. J Trauma Acute Care Surg. 2012. PMID: 22847082 Free PMC article.
-
Reducing noninfectious risks of blood transfusion.Anesthesiology. 2011 Sep;115(3):635-49. doi: 10.1097/ALN.0b013e31822a22d9. Anesthesiology. 2011. PMID: 21792054 Free PMC article. Review.
References
-
- American College of Surgeons Committee on Trauma (1997) Advanced trauma life support course for doctors. Chicago, American College of Surgeons, pp 87–107
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
