

New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality
- PMID: 19454409
- PMCID: PMC2782114
- DOI: 10.1136/thx.2008.109785
New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality
Abstract
Background: The database of the German programme for quality in healthcare including data of every hospitalised patient with community-acquired pneumonia (CAP) during a 2-year period (n = 388 406 patients in 2005 and 2006) was analysed.
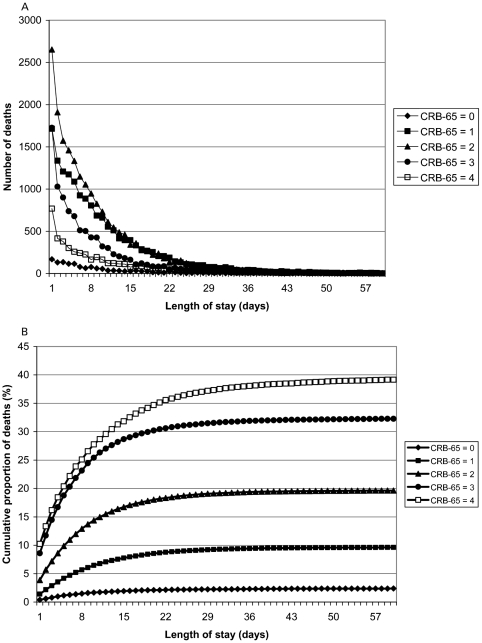
Methods: End points of the analysis were: (1) incidence; (2) outcome; (3) performance of the CRB-65 (C, mental confusion; R, respiratory rate >or=30/min; B, systolic blood pressure <90 mm Hg or diastolic blood pressure <or=60 mm Hg; 65, age >or=65 years) score in predicting death; and (4) lack of ventilatory support as a possible indicator of treatment restrictions. The CRB-65 score was calculated, resulting in three risk classes (RCs).
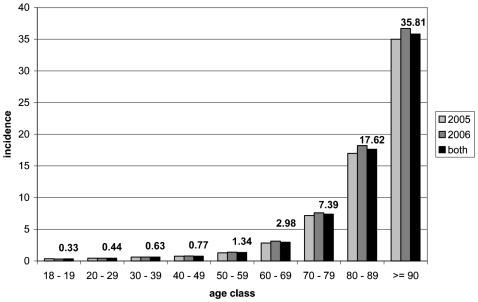
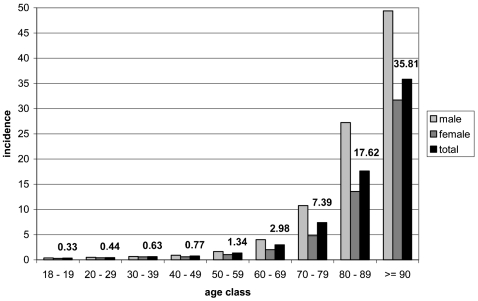
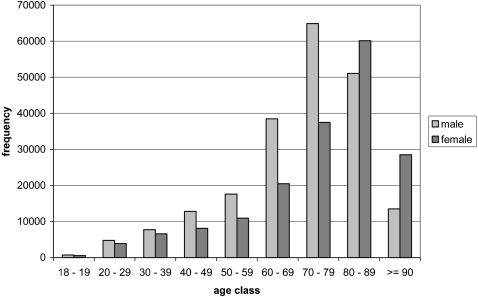
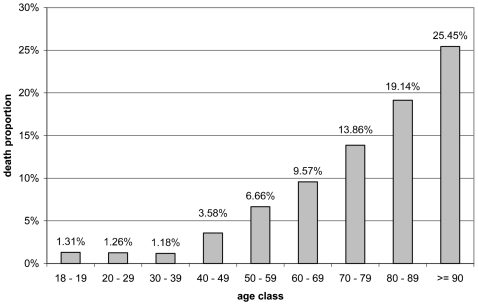
Results: The incidence of hospitalised CAP was 2.75 and 2.96 per 1000 inhabitants/year in 2005 and 2006, respectively, higher for males (3.21 vs 2.52), and strongly age related, with an incidence of 7.65 per 1000 inhabitants/year in patients aged >or=60 years over 2 years. Mortality (13.72% and 14.44%) was higher than reported in previous studies. The CRB-65 RCs accurately predicted death in a three-class pattern (mortality 2.40% in CRB-65 RC 1, 13.43% in CRB-65 RC 2 and 34.39% in CRB-65 RC 3). The first days after admission were consistently associated with the highest risk of death throughout all risk classes. Only a minority of patients who died had received mechanical ventilation during hospitalisation (15.74%).
Conclusions: Hospitalised CAP basically is a condition of the elderly associated with a higher mortality than previously reported. It bears a considerable risk of early mortality, even in low risk patients. CRB-65 is a simple and powerful tool for the assessment of CAP severity. Hospitalised CAP is a frequent terminal event in chronic debilitated patients, and a limitation of treatment escalation is frequently applied.
Conflict of interest statement
None.
Figures
Comment in
-
Meeting the old man's friend.Thorax. 2009 Dec;64(12):1016-7. doi: 10.1136/thx.2009.118299. Thorax. 2009. PMID: 19952230 No abstract available.
-
Predicting CAP-related mortality with CRB-65.Thorax. 2011 Mar;66(3):262; author reply 262-3. doi: 10.1136/thx.2009.133884. Epub 2010 Oct 14. Thorax. 2011. PMID: 20947893 No abstract available.
References
-
- Woodhead M, Blasi F, Ewig S, et als Guidelines for the management of adult lower respiratory tract infections. Eur Respir J 2005;26:1138–80 - PubMed
-
- Höffken G, Lorenz J, Kern W, et al. Epidemiologie, Diagnostik, antimikrobielle Therapie und Management von erwachsenen Patienten mit ambulant erworbenen tiefen Atemwegsinfektionen (akute Bronchitis, akute Exazerbation einer chronischen Bronchitis, Influenza und andere respiratorische Virusinfektionen) sowie ambulant erworbener Pneumonie. Pneumologie 2005;59:612–64
-
- Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997;336:243–50 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous