

Effect of Alemtuzumab (CAMPATH 1-H) in patients with inclusion-body myositis
- PMID: 19454532
- PMCID: PMC2685923
- DOI: 10.1093/brain/awp104
Effect of Alemtuzumab (CAMPATH 1-H) in patients with inclusion-body myositis
Abstract
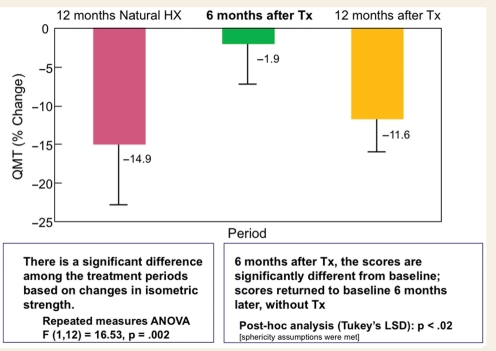
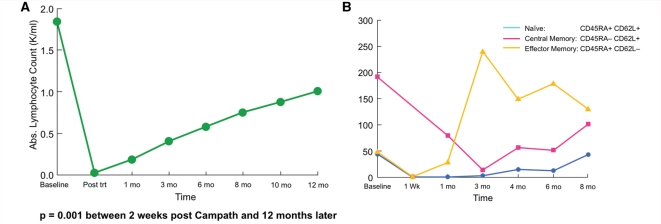
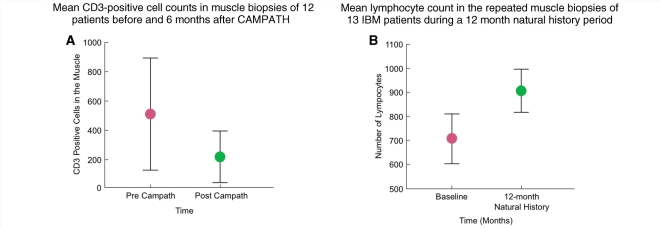
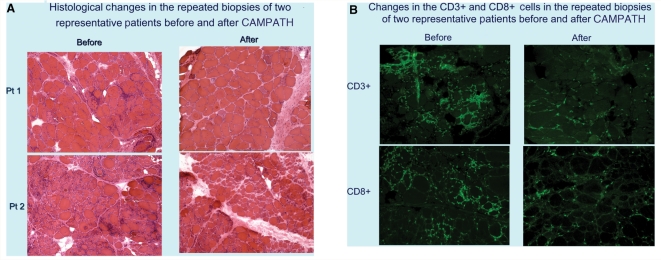
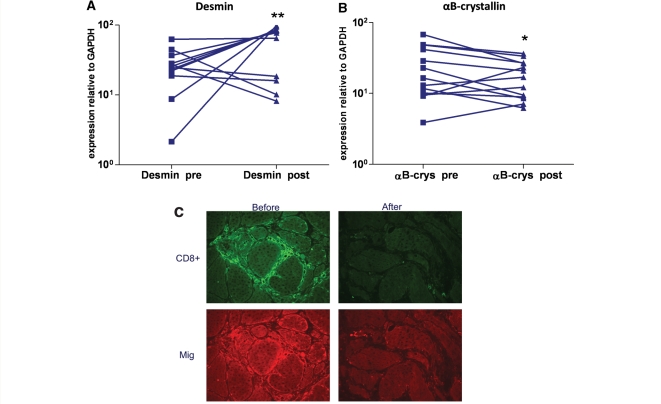
Sporadic inclusion-body myositis (sIBM) is the most common disabling, adult-onset, inflammatory myopathy histologically characterized by intense inflammation and vacuolar degeneration. In spite of T cell-mediated cytotoxicity and persistent, clonally expanded and antigen-driven endomysial T cells, the disease is resistant to immunotherapies. Alemtuzumab is a humanized monoclonal antibody that causes an immediate depletion or severe reduction of peripheral blood lymphocytes, lasting at least 6 months. We designed a proof-of-principle study to examine if one series of Alemtuzumab infusions in sIBM patients depletes not only peripheral blood lymphocytes but also endomysial T cells and alters the natural course of the disease. Thirteen sIBM patients with established 12-month natural history data received 0.3 mg/kg/day Alemtuzumab for 4 days. The study was powered to capture > or =10% increase strength 6 months after treatment. The primary end-point was disease stabilization compared to natural history, assessed by bi-monthly Quantitative Muscle Strength Testing and Medical Research Council strength measurements. Lymphocytes and T cell subsets were monitored concurrently in the blood and the repeated muscle biopsies. Alterations in the mRNA expression of inflammatory, stressor and degeneration-associated molecules were examined in the repeated biopsies. During a 12-month observation period, the patients' total strength had declined by a mean of 14.9% based on Quantitative Muscle Strength Testing. Six months after therapy, the overall decline was only 1.9% (P < 0.002), corresponding to a 13% differential gain. Among those patients, four improved by a mean of 10% and six reported improved performance of daily activities. The benefit was more evident by the Medical Research Council scales, which demonstrated a decline in the total scores by 13.8% during the observation period but an improvement by 11.4% (P < 0.001) after 6 months, reaching the level of strength recorded 12 months earlier. Depletion of peripheral blood lymphocytes, including the naive and memory CD8+ cells, was noted 2 weeks after treatment and persisted up to 6 months. The effector CD45RA(+)CD62L(-) cells, however, started to increase 2 months after therapy and peaked by the 4th month. Repeated muscle biopsies showed reduction of CD3 lymphocytes by a mean of 50% (P < 0.008), most prominent in the improved patients, and reduced mRNA expression of stressor molecules Fas, Mip-1a and alphaB-crystallin; the mRNA of desmin, a regeneration-associated molecule, increased. This proof-of-principle study provides insights into the pathogenesis of inclusion-body myositis and concludes that in sIBM one series of Alemtuzumab infusions can slow down disease progression up to 6 months, improve the strength of some patients, and reduce endomysial inflammation and stressor molecules. These encouraging results, the first in sIBM, warrant a future study with repeated infusions
Trial registration: ClinicalTrials.gov NCT00079768.
Figures

Comment in
-
Comment on alemtuzumab and inclusion body myositis.Brain. 2010 May;133(Pt 5):e135; author reply e136. doi: 10.1093/brain/awp275. Epub 2009 Nov 5. Brain. 2010. PMID: 19892769 Free PMC article. No abstract available.
References
-
- Armstrong N, Buckley P, Oberley T, Fechner J, Jr, Dong Y, Hong X, et al. Analysis of primate renal allografts following T cell depletion with anti-CD3-CRM9. Transplantation. 1998;66:5–13. - PubMed
-
- Askanas V, Engel WK. Inclusion-body myositis: a myodegenerative conformational disorder associated with Abeta, protein misfolding, and proteasome inhibition. Neurology. 2006;66(2 Suppl 1):S39–48. - PubMed
-
- Badrising UA, Schreuder GM, Giphart MJ, Geleijns K, Verschuuren JJ, Wintzen AR, et al. Associations with autoimmune disorders and HLA class I and II antigens in inclusion body myositis. Neurology. 2004;63:2396–8. - PubMed
-
- Banwell BL, Engel AG. AlphaB-crystallin immunolocalization yields new insights into inclusion body myositis. Neurology. 2000;54:1033–41. - PubMed
-
- Chahin N, Engel AG. Correlation of muscle biopsy, clinical course, and outcome in PM and sporadic IBM. Neurology. 2008;70:418–24. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
