

Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial
- PMID: 19454639
- PMCID: PMC3050624
- DOI: 10.1001/jama.2009.682
Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial
Abstract
Context: Cognitive behavioral therapy (CBT) and hypnotic medications are efficacious for short-term treatment of insomnia, but few patients achieve complete remission with any single treatment. It is unclear whether combined or maintenance therapies would enhance outcome.
Objectives: To evaluate the added value of medication over CBT alone for acute treatment of insomnia and the effects of maintenance therapies on long-term outcome.
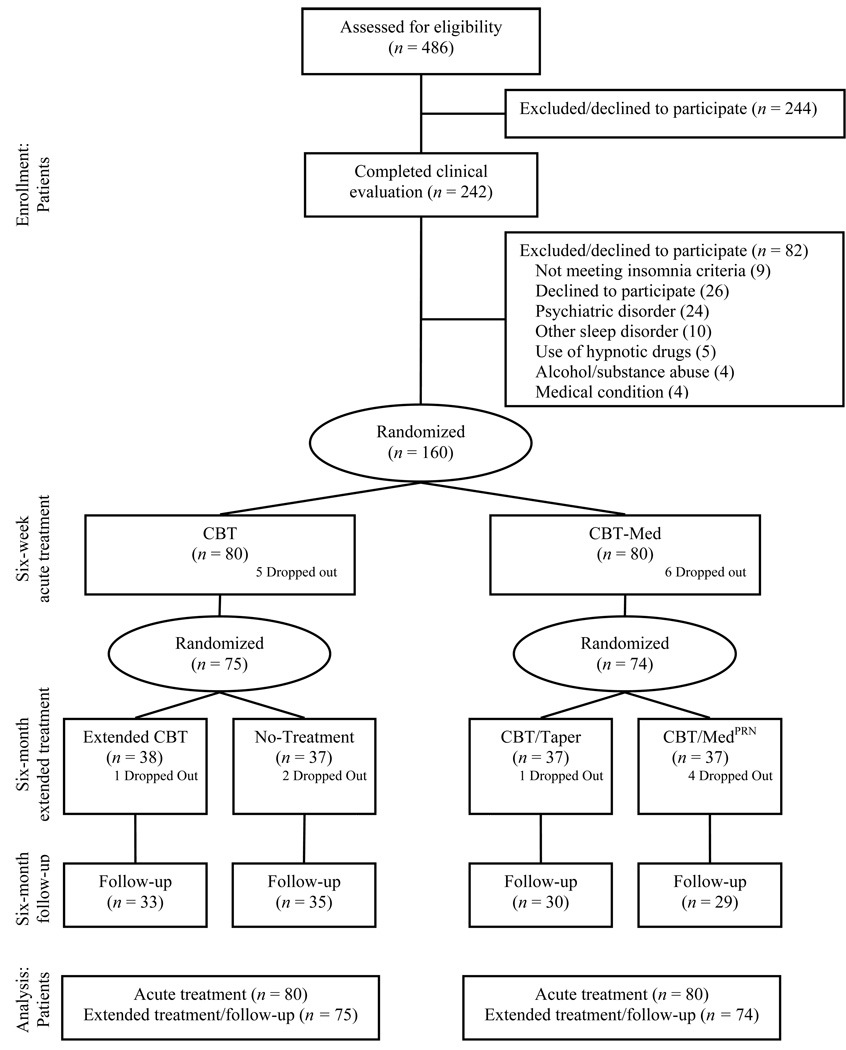
Design, setting, and patients: Prospective, randomized controlled trial involving 2-stage therapy for 160 adults with persistent insomnia treated at a university hospital sleep center in Canada between January 2002 and April 2005.
Interventions: Participants received CBT alone or CBT plus 10 mg/d (taken at bedtime) of zolpidem for an initial 6-week therapy, followed by extended 6-month therapy. Patients initially treated with CBT attended monthly maintenance CBT for 6 months or received no additional treatment and those initially treated with combined therapy (CBT plus 10 mg/d of zolpidem) continued with CBT plus intermittent use of zolpidem or CBT only.
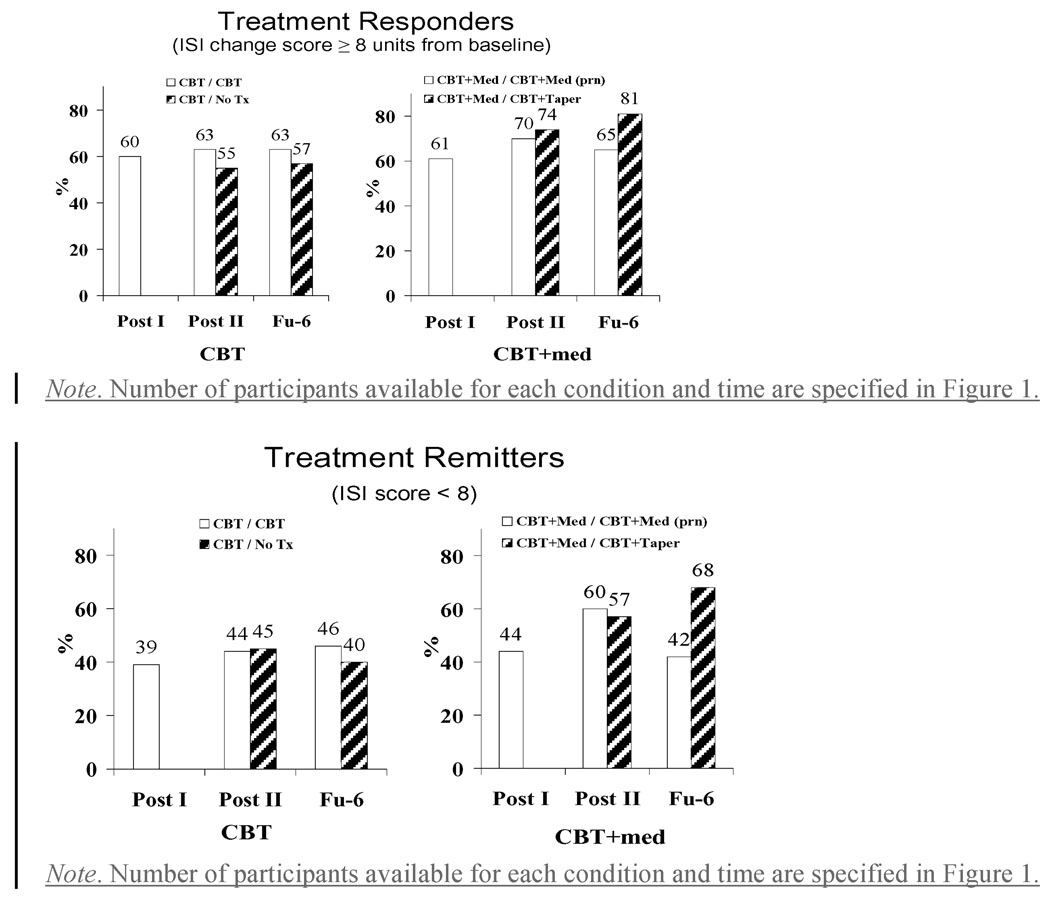
Main outcome measures: Sleep onset latency, time awake after sleep onset, total sleep time, and sleep efficiency derived from daily diaries (primary outcomes); treatment response and remission rates derived from the Insomnia Severity Index (secondary outcomes).
Results: Cognitive behavioral therapy used singly or in combination with zolpidem produced significant improvements in sleep latency, time awake after sleep onset, and sleep efficiency during initial therapy (all P<.001); a larger increase of sleep time was obtained with the combined approach (P = .04). Both CBT alone and CBT plus zolpidem produced similar rates of treatment responders (60% [45/75] vs 61% [45/74], respectively; P = .84) and treatment remissions (39% [29/75] vs 44% [33/74], respectively; P = .52) with the 6-week acute treatment, but combined therapy produced a higher remission rate compared with CBT alone during the 6-month extended therapy phase and the 6-month follow-up period (56% [43/74 and 32/59] vs 43% [34/75 and 28/68]; P = .05). The best long-term outcome was obtained with patients treated with combined therapy initially, followed by CBT alone, as evidenced by higher remission rates at the 6-month follow-up compared with patients who continued to take zolpidem during extended therapy (68% [20/30] vs 42% [12/29]; P = .04).
Conclusion: In patients with persistent insomnia, the addition of medication to CBT produced added benefits during acute therapy, but long-term outcome was optimized when medication is discontinued during maintenance CBT.
Trial registration: clinicaltrials.gov Identifier: NCT00042146.
Figures
Comment in
-
Cognitive behavioral therapy alone and with medication for persistent insomnia.JAMA. 2009 Sep 9;302(10):1053; author reply 1054. doi: 10.1001/jama.2009.1283. JAMA. 2009. PMID: 19738085 No abstract available.
-
Cognitive behavioral therapy alone and with medication for persistent insomnia.JAMA. 2009 Sep 9;302(10):1053; author reply 1054. doi: 10.1001/jama.2009.1282. JAMA. 2009. PMID: 19738086 No abstract available.
-
Adding zolpidem to CBT produces limited benefits in persistent insomnia.Evid Based Ment Health. 2010 Feb;13(1):28. doi: 10.1136/ebmh.13.1.28. Evid Based Ment Health. 2010. PMID: 20164525 No abstract available.
References
-
- Morin CM, LeBlanc M, Daley M, Gregoire JP, Merette C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Medicine. 2006 Mar;7(2):123–130. - PubMed
-
- Ohayon MM. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Medicine Reviews. 2002;6(2):97–111. - PubMed
-
- Daley M, Morin CM, Leblanc M, Gregoire JP, Savard J, Baillargeon L. Insomnia and its relationship to health-care utilization, work absenteeism, productivity and accidents. Sleep Medicine. 2008 Aug 25; - PubMed
-
- Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? Journal of the American Medical Association. 1989;262(11):1479–1484. - PubMed
-
- Ozminkowski RJ, Wang S, Walsh JK. The direct and indirect costs of untreated insomnia in adults in the United States. Sleep. 2007 Mar 1;30(3):263–273. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
