

In-hospital versus out-of-hospital pediatric cardiac arrest: a multicenter cohort study
- PMID: 19455024
- PMCID: PMC2711020
- DOI: 10.1097/CCM.0b013e3181a00a6a
In-hospital versus out-of-hospital pediatric cardiac arrest: a multicenter cohort study
Abstract
Objectives: : To describe a large multicenter cohort of pediatric cardiac arrest (CA) with return of circulation (ROC) from either the in-hospital (IH) or the out-of-hospital (OH) setting and to determine whether significant differences related to pre-event, arrest event, early postarrest event characteristics, and outcomes exist that would be critical in planning a clinical trial of therapeutic hypothermia (TH).
Design: : Retrospective cohort study.
Setting: : Fifteen Pediatric Emergency Care Applied Research Network sites.
Patients: : Patients aged 24 hours to 18 years with either IH or OH CA who had a history of at least 1 minute of chest compressions and ROC for at least 20 minutes were eligible.
Interventions: : None.
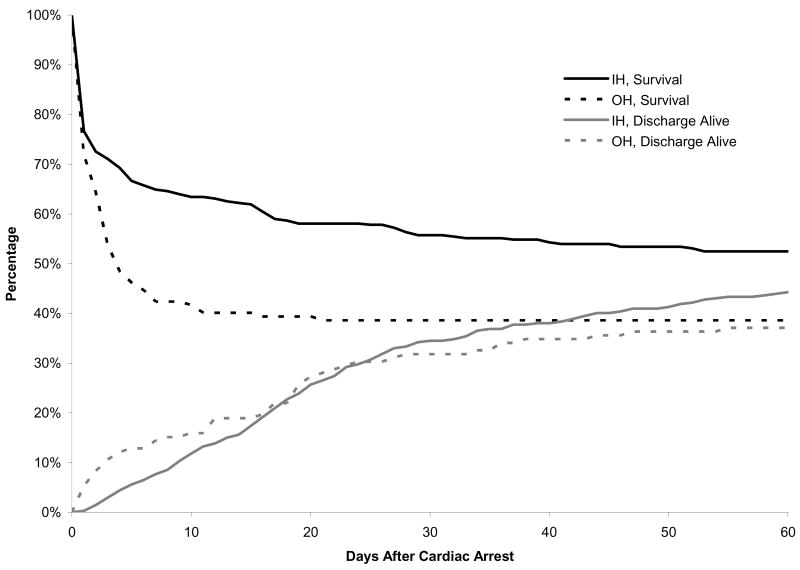
Measurements and main results: : A total of 491 patients met study entry criteria with 353 IH cases and 138 OH cases. Major differences between the IH and OH cohorts were observed for patient prearrest characteristics, arrest event initial rhythm described, and arrest medication use. Several postarrest interventions were used differently, however, the use of TH was similar (<5%) in both cohorts. During the 0-12-hour interval following ROC, OH cases had lower minimum temperature and pH, and higher maximum serum glucose recorded. Mortality was greater in the OH cohort (62% vs. 51%, p = 0.04) with the cause attributed to a neurologic indication much more frequent in the OH than in the IH cohort (69% vs. 20%; p < 0.01).
Conclusions: : For pediatric CA with ROC, several major differences exist between IH and OH cohorts. The finding that the etiology of death was attributed to neurologic indications much more frequently in OH arrests has important implications for future research. Investigators planning to evaluate the efficacy of new interventions, such as TH, should be aware that the IH and OH populations differ greatly and require independent clinical trials.
Figures
Comment in
-
Cardiopulmonary resuscitation in childhood: understanding how to give better treatment and improve outcome.Crit Care Med. 2009 Jul;37(7):2318-9. doi: 10.1097/CCM.0b013e3181a5c260. Crit Care Med. 2009. PMID: 19535933 No abstract available.
References
-
- Young KD, Seidel JS. Pediatric cardiopulmonary resuscitation: a collective review. Ann Emer Med. 1999;33:195–205. - PubMed
-
- Donoghue AG, Nadkarni V, Berg RA, et al. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med. 2005;46:512–22. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. for the National Registry of Cardiopulmonary Resuscitation Investigators. First Documented Rhythm and Clinical Outcome from In-Hospital Cardiac Arrest Among Children and Adults. JAMA. 2006;295:50–57. - PubMed
-
- Young KD, Gausche-Hill M, McClung CD, Lewis RJ. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics. 2004;114:157–164. - PubMed
-
- Sirbaugh PE, Pepe PE, Shook JE, et al. A prospective, population-based study of the demographics, epidemiology, management, and outcome of out-of-hospital pediatric cardiopulmonary arrest. Ann Emerg Med. 1999;33:174–184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
