

Review
doi: 10.1583/08-2583.1.
Clinical significance and technical assessment of stent cell geometry in carotid artery stenting
Affiliations
- PMID: 19456193
- PMCID: PMC5621709
- DOI: 10.1583/08-2583.1
Item in Clipboard
Review
Clinical significance and technical assessment of stent cell geometry in carotid artery stenting
J Endovasc Ther.
2009 Apr.
Abstract
Carotid artery stenting has gained popularity due to its minimally invasive approach. However, several design concerns preclude the successful use of carotid stents. Technical issues, such as open versus closed cells, scaffolding, trackability, foreshortening, and changes in local geometry and hemodynamics, affect stent performance. Previous clinical and experimental studies have evaluated current stent models while proposing and testing novel stent designs. This review focuses on the technical aspects of carotid stent design and the clinical significance of key design parameters identified via computational and experimental modeling.
Figures

Cross section of a specimen demonstrating a balloon-expandable stent with excellent apposition and plaque scaffolding.

(A) A significant stenotic lesion with major ulceration in the right ICA (B) effectively managed with a stent precisely positioned at the ostium.

First-generation Palmaz-Schatz stent demonstrating the bridge that allowed increased length with flexibility.

Closed-cell design with a detailed view of the bridge (arrows) demonstrating flexibility and conformability after expansion.

(A) Closed-cell stent demonstrating the diamond configuration with radial segments and bridge connection (arrow); (B) open-cell stent with removal of a bridge connection illustrated.

(A) Fully supported closed-cell stent, demonstrating comparable flexibility to the (B) unsupported open-cell stent.

(A) Larger open-cell design stents may not provide adequate scaffolding in a complex bend, but do provide conformability. (B) Open-cell design at the concave surface of the stent showing scaling. (C) Post-procedure angiogram demonstrating the open-cell struts extending beyond the intima, with focal contrast extravasation to the adventitia.

Strut fracture in a nitinol carotid stent as seen on a 3-dimensional reconstructed angiogram.

Stent configurations in a carotid glass model with variations in conformability: (from left to right) NexStent, Wallstent, and Precise stents.
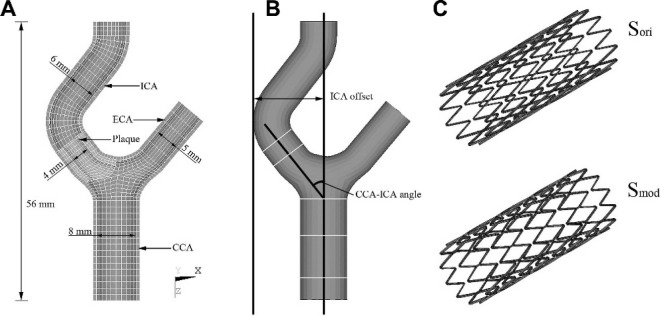
(A) Cross section of the carotid artery. CCA: common carotid artery, ICA: internal carotid artery, ECA: external carotid artery. (B) The CCA-ICA angle of the vessel, which reflects ICA tortuosity. (C) The segmented nitinol stent models Sori and Smod. Reproduced with permission from Journal of Biomechanics. Copyright 2007 Elsevier.

Design parameters for a generic stent showing the 3 parameters identified by the optimization algorithm: strut spacing (h), radius of curvature (ρ), and axial amplitude (f). Reproduced with permission from Medical and Biological Engineering and Computing. Copyright 2007 Springer.

(A) Virtual histology images at 3 sites in a carotid artery demonstrating lesion characteristics that are best suited for endarterectomy rather than stenting. Note the absence of any fibrous cap and the exposure to the necrotic core at the intimal surface. (B) Pre-occlusive ICA lesion with complex ulceration and angulation. (C) Virtual histology of the lesion demonstrating significant necrotic core and dystrophic calcification at the intimal surface. These lesion characteristics are best suited for endarterectomy.

(A) A high-grade stenotic lesion with ulcerative changes best suited for a closed-cell stent; (B) post-procedure angiogram showing flow pathway restored.
References
-
- Wholey MH, Al-Mubarak N, Wholey MH. Updated review of the global carotid artery stent registry. Catheter Cardiovasc Interv. 2003;60:259–266. - PubMed
-
- Palmaz JC. Intravascular stents in the last and the next 10 years. J Endovasc Ther. 2004;11(Suppl II):II-200–II-206. - PubMed
-
- Wentzel JJ, Whelan DM, van der Giessen WJ, et al. Coronary stent implantation changes 3-D vessel geometry and 3-D shear stress distribution. J Biomech. 2000;33:1287–1295. - PubMed
-
- Duraiswamy N, Schoephoerster RT, Moreno MR, et al. Stented artery flow patterns and their effects on the artery wall. Annu Rev Fluid Mech. 2007;39:357–382.
-
- Hart JP, Peeters P, Verbist J, et al. Do device characteristics impact outcome in carotid artery stenting? J Vasc Surg. 2006;44:725–731. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
