

Effect of dipyridamole plus aspirin on hemodialysis graft patency
- PMID: 19458364
- PMCID: PMC3929400
- DOI: 10.1056/NEJMoa0805840
Effect of dipyridamole plus aspirin on hemodialysis graft patency
Abstract
Background: Arteriovenous graft stenosis leading to thrombosis is a major cause of complications in patients undergoing hemodialysis. Procedural interventions may restore patency but are costly. Although there is no proven pharmacologic therapy, dipyridamole may be promising because of its known vascular antiproliferative activity.
Methods: We conducted a randomized, double-blind, placebo-controlled trial of extended-release dipyridamole, at a dose of 200 mg, and aspirin, at a dose of 25 mg, given twice daily after the placement of a new arteriovenous graft until the primary outcome, loss of primary unassisted patency (i.e., patency without thrombosis or requirement for intervention), was reached. Secondary outcomes were cumulative graft failure and death. Primary and secondary outcomes were analyzed with the use of a Cox proportional-hazards regression with adjustment for prespecified covariates.
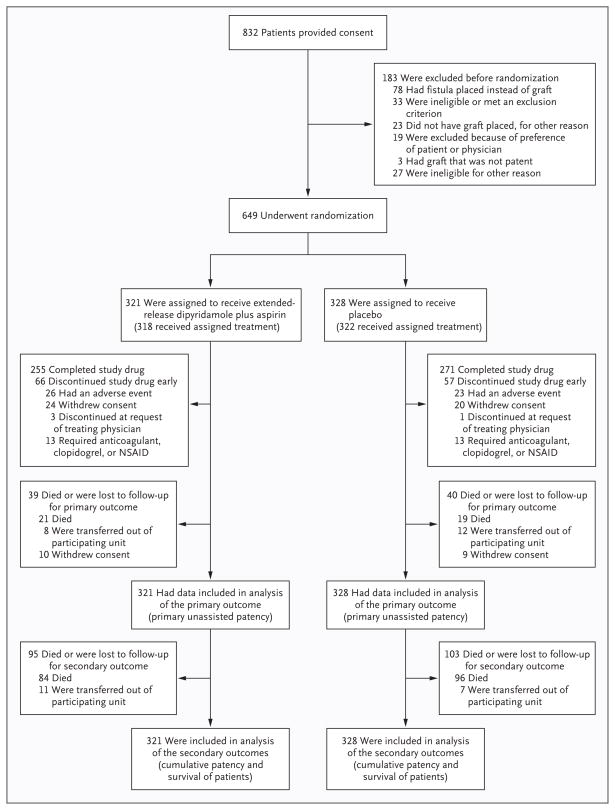
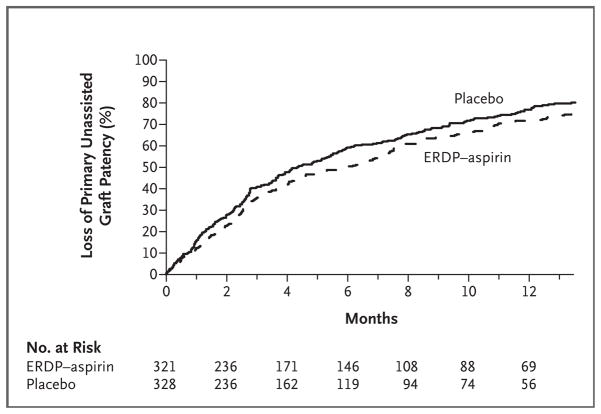
Results: At 13 centers in the United States, 649 patients were randomly assigned to receive dipyridamole plus aspirin (321 patients) or placebo (328 patients) over a period of 4.5 years, with 6 additional months of follow-up. The incidence of primary unassisted patency at 1 year was 23% (95% confidence interval [CI], 18 to 28) in the placebo group and 28% (95% CI, 23 to 34) in the dipyridamole-aspirin group, an absolute difference of 5 percentage points. Treatment with dipyridamole plus aspirin significantly prolonged the duration of primary unassisted patency (hazard ratio, 0.82; 95% CI, 0.68 to 0.98; P=0.03) and inhibited stenosis. The incidences of cumulative graft failure, death, the composite of graft failure or death, and serious adverse events (including bleeding) did not differ significantly between study groups.
Conclusions: Treatment with dipyridamole plus aspirin had a significant but modest effect in reducing the risk of stenosis and improving the duration of primary unassisted patency of newly created grafts. (ClinicalTrials.gov number, NCT00067119.)
2009 Massachusetts Medical Society
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Antiplatelet therapy and vascular-access patency.N Engl J Med. 2009 May 21;360(21):2240-2. doi: 10.1056/NEJMe0902841. N Engl J Med. 2009. PMID: 19458370 No abstract available.
-
Dipyridamole plus aspirin and hemodialysis graft patency.N Engl J Med. 2009 Aug 13;361(7):720; author reply 721. doi: 10.1056/NEJMc091312. N Engl J Med. 2009. PMID: 19675337 No abstract available.
-
Dipyridamole plus aspirin and hemodialysis graft patency.N Engl J Med. 2009 Aug 13;361(7):720-1; author reply 721. N Engl J Med. 2009. PMID: 19681176 No abstract available.
References
-
- Feldman HI, Kobrin S, Wasserstein A. Hemodialysis vascular access morbidity. J Am Soc Nephrol. 1996;7:523–35. - PubMed
-
- U.S. Renal Data System. 2006 Annual data report: atlas of end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2006.
-
- Roy-Chaudhury P, Sukhatme VP, Cheung AK. Hemodialysis vascular access dysfunction: a cellular and molecular viewpoint. J Am Soc Nephrol. 2006;17:1112–27. - PubMed
-
- Gibson KD, Gillen DL, Caps MT, Kohler TR, Sherrard DJ, Stehman-Breen CO. Vascular access survival and incidence of revisions: a comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States Renal Data System Dialysis Morbidity and Mortality Study. J Vasc Surg. 2001;34:694–700. - PubMed
-
- U.S. Renal Data System. 2007 Annual data report: atlas of end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2007.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 DK058982/DK/NIDDK NIH HHS/United States
- U01 DK058986/DK/NIDDK NIH HHS/United States
- U01DK058978/DK/NIDDK NIH HHS/United States
- U01DK058985/DK/NIDDK NIH HHS/United States
- U01DK058986/DK/NIDDK NIH HHS/United States
- U01 DK058973/DK/NIDDK NIH HHS/United States
- U01DK058966/DK/NIDDK NIH HHS/United States
- U01 DK058966/DK/NIDDK NIH HHS/United States
- U01 DK058981/DK/NIDDK NIH HHS/United States
- U01DK058982/DK/NIDDK NIH HHS/United States
- U01 DK058968/DK/NIDDK NIH HHS/United States
- U01DK058973/DK/NIDDK NIH HHS/United States
- U01 DK058978/DK/NIDDK NIH HHS/United States
- U01DK058981/DK/NIDDK NIH HHS/United States
- U01 DK058985/DK/NIDDK NIH HHS/United States
- U01DK058968/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical