

Similar outcomes with different rates of delayed graft function may reflect center practice, not center performance
- PMID: 19459804
- PMCID: PMC2758075
- DOI: 10.1111/j.1600-6143.2009.02651.x
Similar outcomes with different rates of delayed graft function may reflect center practice, not center performance
Abstract
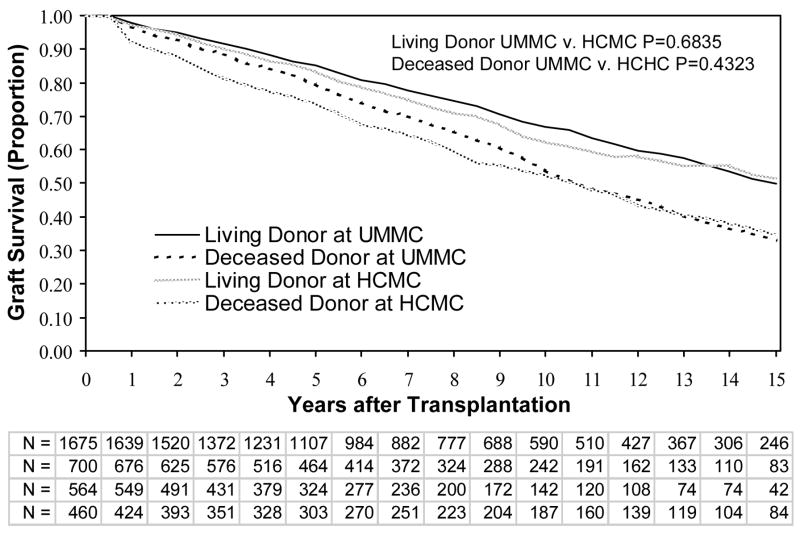
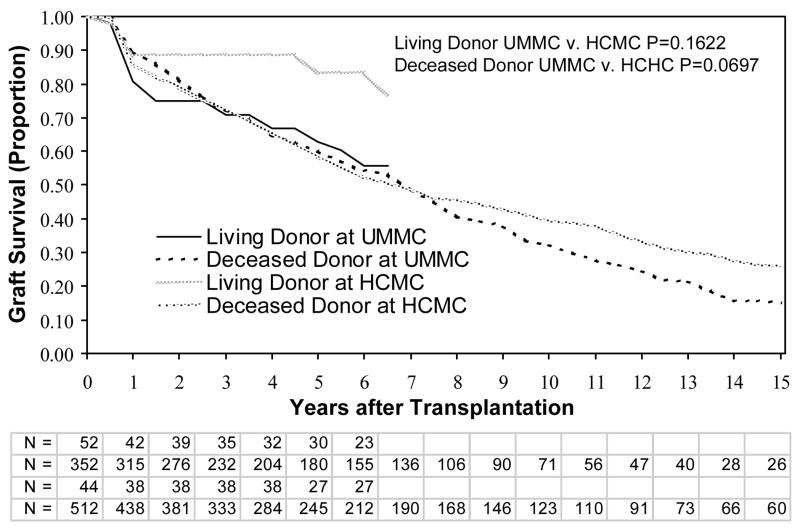
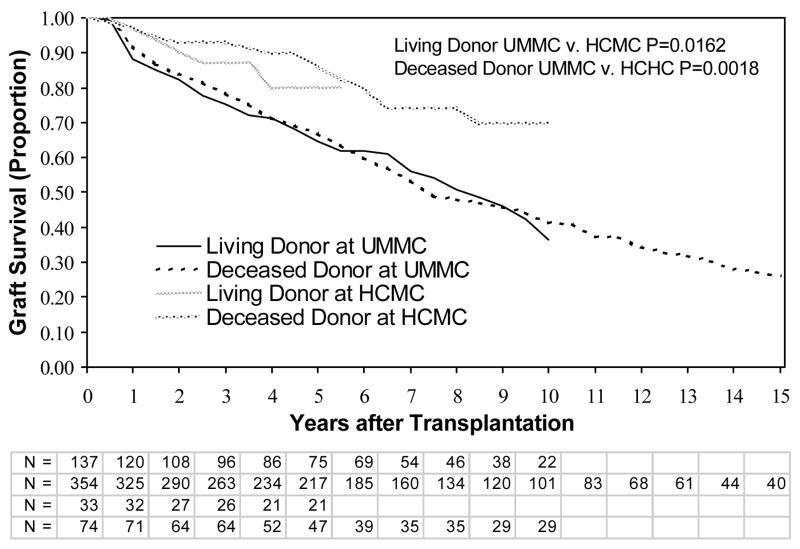
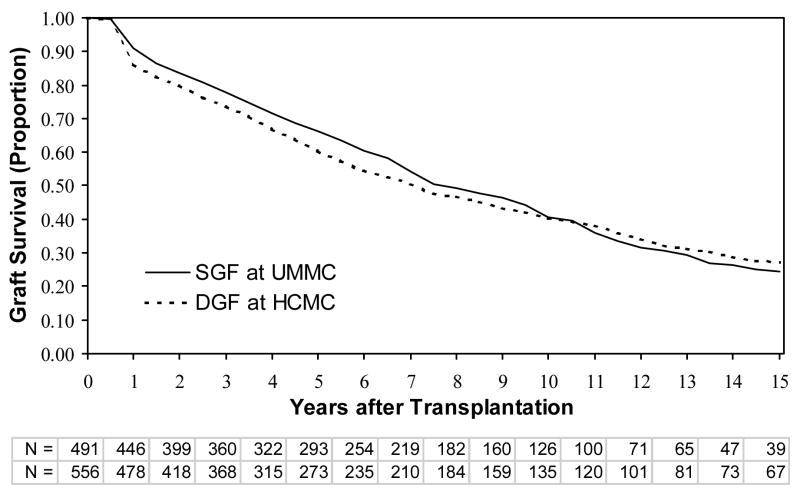
To better understand the implications for considering delayed graft function (DGF) as a performance measure, we compared outcomes associated with a 2- to 3-fold difference in the incidence of DGF at two transplant centers. We analyzed 5072 kidney transplantations between 1984 and 2006 at the University of Minnesota Medical Center (UMMC) and Hennepin County Medical Center (HCMC). In logistic regression the adjusted odds ratio for DGF at HCMC versus UMMC was 3.11 (95% Confidence Interval [CI]= 2.49-3.89) for deceased donors and 2.24 (CI = 1.45-3.47) for living donors. In Cox analysis of 4957 transplantations, slow graft function (SGF; creatinine >or=3.0 mg/dL [230 micromol/L] on day 5 without dialysis) was associated with graft failure at UMMC (Relative Risk [RR]= 1.43, CI = 1.25-1.64), but not HCMC (RR = 0.99, CI = 0.77-1.28). RR's of DGF were similar at both centers. Thus, the lower incidence of DGF at UMMC likely resulted in a higher incidence and higher risk of SGF compared to HCMC. Indeed, graft survival for recipients with DGF at HCMC was similar (p = 0.3741) to that of recipients with SGF at UMMC. We conclude that dialysis per se is likely not a cause of worse graft outcomes. A better definition is needed to measure early graft dysfunction and its effects across transplant programs.
Figures
References
-
- Ojo AO, Wolfe RA, Held PJ, Port FK, Schmouder RL. Delayed graft function: risk factors and implications for renal allograft survival. Transplantation. 1997;63(7):968–974. - PubMed
-
- Cecka JM. The UNOS Scientific Regristry. In: Cecka JM, Terasaki PI, editors. Clinical Transplants 1998. Los Angeles: UCLA Tissue Typing Laboratory; 1999. pp. 1–16.
-
- Shoskes DA, Cecka JM. Deleterious effects of delayed graft function in cadaveric renal transplant recipients independent of acute rejection. Transplantation. 1998;66(12):1697–1701. - PubMed
-
- Feldman HI, Gayner R, Berlin JA, Roth DA, Silibovsky R, Kushner S, et al. Delayed function reduces renal allograft survival independent of acute rejection. Nephrol Dial Transplant. 1996;11(7):1306–1313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
