

Comparison of spirometry criteria for the diagnosis of COPD: results from the BOLD study
- PMID: 19460786
- PMCID: PMC3334278
- DOI: 10.1183/09031936.00164608
Comparison of spirometry criteria for the diagnosis of COPD: results from the BOLD study
Abstract
Published guidelines recommend spirometry to accurately diagnose chronic obstructive pulmonary disease (COPD). However, even spirometry-based COPD prevalence estimates can vary widely. We compared properties of several spirometry-based COPD definitions using data from the international Burden of Obstructive Lung Disease (BOLD)study. 14 sites recruited population-based samples of adults aged > or =40 yrs. Procedures included standardised questionnaires and post-bronchodilator spirometry. 10,001 individuals provided usable data. Use of the lower limit of normal (LLN) forced expiratory volume in 1 s (FEV(1)) to forced vital capacity (FVC) ratio reduced the age-related increases in COPD prevalence that are seen among healthy never-smokers when using the fixed ratio criterion (FEV(1)/FVC <0.7) recommended by the Global Initiative for Chronic Obstructive Lung Disease. The added requirement of an FEV(1) either <80% predicted or below the LLN further reduced age-related increases and also led to the least site-to-site variability in prevalence estimates after adjusting for potential confounders. Use of the FEV(1)/FEV(6) ratio in place of the FEV(1)/FVC yielded similar prevalence estimates. Use of the FEV(1)/FVC<LLN criterion instead of the FEV(1)/FVC <0.7 should minimise known age biases and better reflect clinically significant irreversible airflow limitation. Our study also supports the use of the FEV(1)/FEV(6) as a practical substitute for the FEV(1)/FVC.
Figures
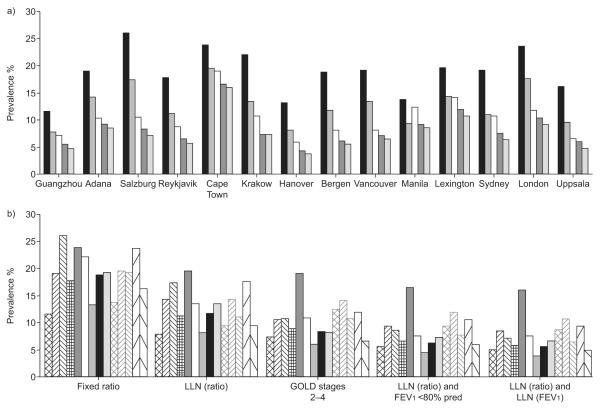
 : lower limit of normal (LLN) (ratio); □: Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages 2–4;
: lower limit of normal (LLN) (ratio); □: Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages 2–4;  : LLN (ratio) and forced expiratory volume in 1 s (FEV1) <80% predicted;
: LLN (ratio) and forced expiratory volume in 1 s (FEV1) <80% predicted;  : LLN (ratio) and LLN (FEV1). b) Contrasting site differences within each definition. Significant site-to-site variability persisted for each of the estimates even after adjusting for age, sex, cigarette smoking (pack-yrs), body mass index, years worked in a dusty job and interactions of sex with both age and smoking history in logistic regression models (Wald statistics ranging from 7.1 to 8.6, all p-values <0.0001). Prevalences based on the fixed ratio are significantly higher than for all other estimators at each site (all p-values <0.001).
: LLN (ratio) and LLN (FEV1). b) Contrasting site differences within each definition. Significant site-to-site variability persisted for each of the estimates even after adjusting for age, sex, cigarette smoking (pack-yrs), body mass index, years worked in a dusty job and interactions of sex with both age and smoking history in logistic regression models (Wald statistics ranging from 7.1 to 8.6, all p-values <0.0001). Prevalences based on the fixed ratio are significantly higher than for all other estimators at each site (all p-values <0.001).  : Guangzhou, China;
: Guangzhou, China;  : Adana, Turkey;
: Adana, Turkey;  : Salzburg, Austria;
: Salzburg, Austria;  : Reykjavik, Iceland;
: Reykjavik, Iceland;  : Cape Town, South Africa; □: Krakow, Poland;
: Cape Town, South Africa; □: Krakow, Poland;  : Hanover, Germany; ■: Bergen, Norway;
: Hanover, Germany; ■: Bergen, Norway;  : Vancouver, BC, Canada;
: Vancouver, BC, Canada;  : Manila, Philippines;
: Manila, Philippines;  : Lexington, KY, USA;
: Lexington, KY, USA;  : Sydney, Australia;
: Sydney, Australia;  : London, UK;
: London, UK;  : Uppsala, Sweden.
: Uppsala, Sweden.

 : NHANES-III; □: Hordaland County; Δ: local equations.
: NHANES-III; □: Hordaland County; Δ: local equations.Comment in
-
Debating the definition of airflow obstruction: time to move on?Eur Respir J. 2009 Sep;34(3):527-8. doi: 10.1183/09031936.00103309. Eur Respir J. 2009. PMID: 19720804 No abstract available.
References
-
- Halbert RJ, Natoli JL, Gano A, et al. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28:523–532. - PubMed
-
- Celli BR, Halbert RJ, Isonaka S, et al. Population impact of different definitions of airway obstruction. Eur Respir J. 2003;22:268–273. - PubMed
-
- Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–555. - PubMed
-
- Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–946. - PubMed
-
- Viegi G, Pedreschi M, Pistelli F, et al. Prevalence of airways obstruction in a general population: European Respiratory Society versus American Thoracic Society definition. Chest. 2000;117:339S–345S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical