

Effects of structured versus usual care on renal endpoint in type 2 diabetes: the SURE study: a randomized multicenter translational study
- PMID: 19460913
- PMCID: PMC2681013
- DOI: 10.2337/dc08-1908
Effects of structured versus usual care on renal endpoint in type 2 diabetes: the SURE study: a randomized multicenter translational study
Abstract
Objective: Multifaceted care has been shown to reduce mortality and complications in type 2 diabetes. We hypothesized that structured care would reduce renal complications in type 2 diabetes.
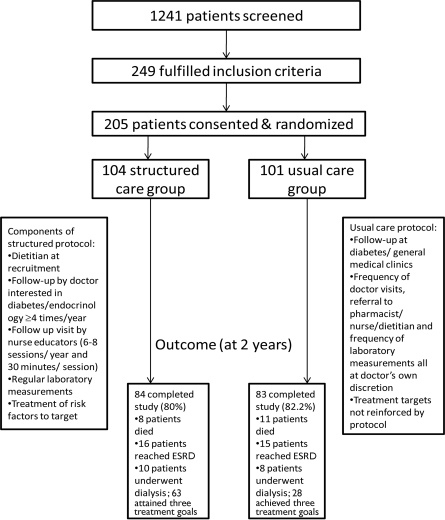
Research design and methods: A total of 205 Chinese type 2 diabetic patients from nine public hospitals who had plasma creatinine levels of 150-350 micromol/l were randomly assigned to receive structured care (n = 104) or usual care (n = 101) for 2 years. The structured care group was managed according to a prespecified protocol with the following treatment goals: blood pressure <130/80 mmHg, A1C <7%, LDL cholesterol <2.6 mmol/l, triglyceride <2 mmol/l, and persistent treatment with renin-angiotensin blockers. The primary end point was death and/or renal end point (creatinine >500 micromol/l or dialysis).
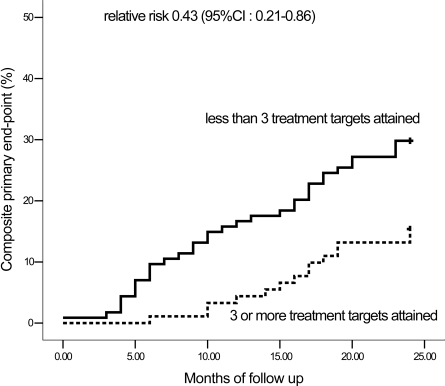
Results: Of these 205 patients (mean +/- SD age 65 +/- 7.2 years; disease duration 14 +/- 7.9 years), the structured care group achieved better control than the usual care group (diastolic blood pressure 68 +/- 12 vs. 71 +/- 12 mmHg, respectively, P = 0.02; A1C 7.3 +/- 1.3 vs. 8.0 +/- 1.6%, P < 0.01). After adjustment for age, sex, and study sites, the structured care (23.1%, n = 24) and usual care (23.8%, n = 24; NS) groups had similar end points, but more patients in the structured care group attained >or=3 treatment goals (61%, n = 63, vs. 28%, n = 28; P < 0.001). Patients who attained >or=3 treatment targets (n = 91) had reduced risk of the primary end point (14 vs. 34; relative risk 0.43 [95% CI 0.21-0.86] compared with that of those who attained <or=2 targets (n = 114).
Conclusions: Attainment of multiple treatment targets reduced the renal end point and death in type 2 diabetes. In addition to protocol, audits and feedback are needed to improve outcomes.
Trial registration: ClinicalTrials.gov NCT00309127.
Figures
Comment in
-
Intensive diabetes management for high-risk patients: how best to deliver?Diabetes Care. 2009 Jun;32(6):1132-3. doi: 10.2337/dc09-0540. Diabetes Care. 2009. PMID: 19460918 Free PMC article. No abstract available.
References
-
- Gaede P, Lund-Andersen H, Parving HH, et al. : Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008; 358: 580– 591 - PubMed
-
- Gaede P, Vedel P, Larsen N, et al. : Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003; 348: 383– 393 - PubMed
-
- So WY, Kong AP, Ma RC, et al. : Glomerular filtration rate, cardiorenal end points, and all-cause mortality in type 2 diabetic patients. Diabetes Care 2006; 29: 2046– 2052 - PubMed
-
- Ritz E, Rychlik I, Locatelli F, et al. : End-stage renal failure in type 2 diabetes: a medical catastrophe of worldwide dimensions. Am J Kidney Dis 1999; 34: 795– 808 - PubMed
-
- So WY, Tong PC, Ko GT, et al. : Effects of protocol-driven care versus usual outpatient clinic care on survival rates in patients with type 2 diabetes. Am J Manag Care 2003; 9: 606– 615 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
