

Short-term and long-term risk of tuberculosis associated with CD4 cell recovery during antiretroviral therapy in South Africa
- PMID: 19461502
- PMCID: PMC3801095
- DOI: 10.1097/QAD.0b013e32832d3b6d
Short-term and long-term risk of tuberculosis associated with CD4 cell recovery during antiretroviral therapy in South Africa
Abstract
Objective: To determine the short-term and long-term risks of tuberculosis (TB) associated with CD4 cell recovery during antiretroviral therapy (ART).
Design: Observational community-based ART cohort in South Africa.
Methods: TB incidence was determined among patients (n = 1480) receiving ART for up to 4.5 years in a South African community-based service. Updated CD4 cell counts were measured 4-monthly. Person-time accrued within a range of CD4 cell count strata (CD4 cell strata) was calculated and used to derive CD4 cell-stratified TB rates. Factors associated with incident TB were identified using Poisson regression models.
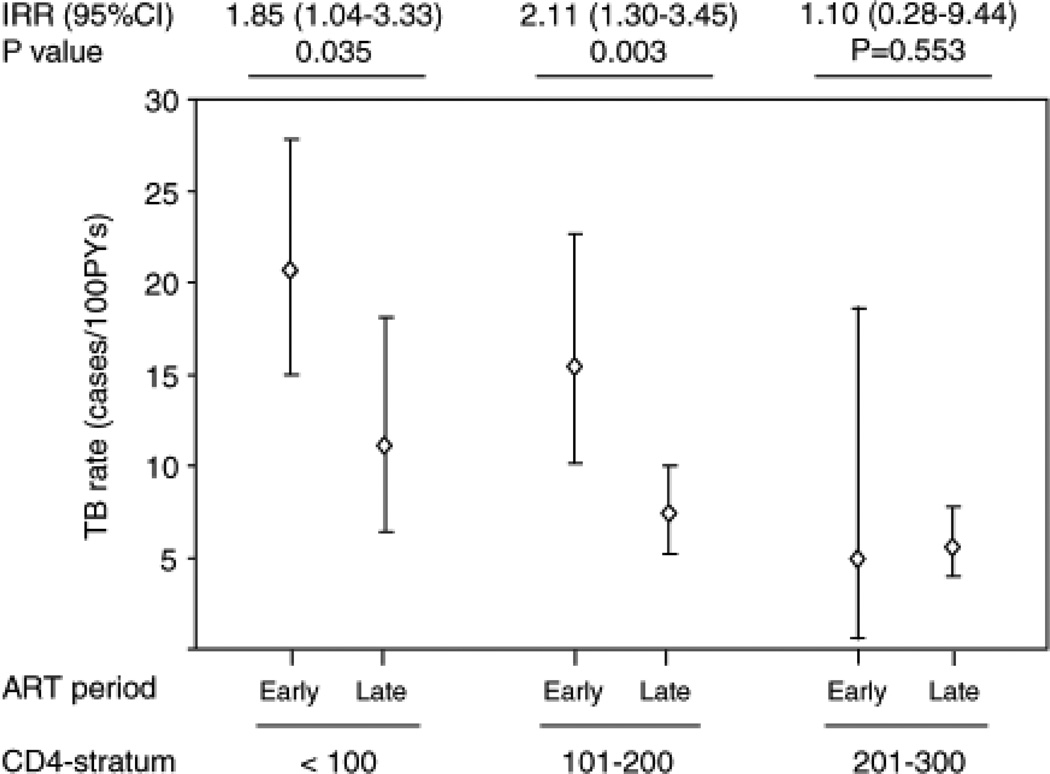
Results: Two hundred and three cases of TB were diagnosed during 2785 person-years of observation (overall incidence, 7.3 cases/100 person-years). During person-time accrued within CD4 cell strata 0-100, 101-200, 201-300, 301-400, 401-500 and more than 500 cells/microl unadjusted TB incidence rates were 16.8, 9.3, 5.5, 4.6, 4.2 and 1.5 cases/100 person-years, respectively (P < 0.001). During early ART (first 4 months), adjusted TB rates among those with CD4 cell counts 0-200 cells/microl were 1.7-fold higher than during long-term ART (P = 0.026). Updated CD4 cell counts were the only patient characteristic independently associated with long-term TB risk.
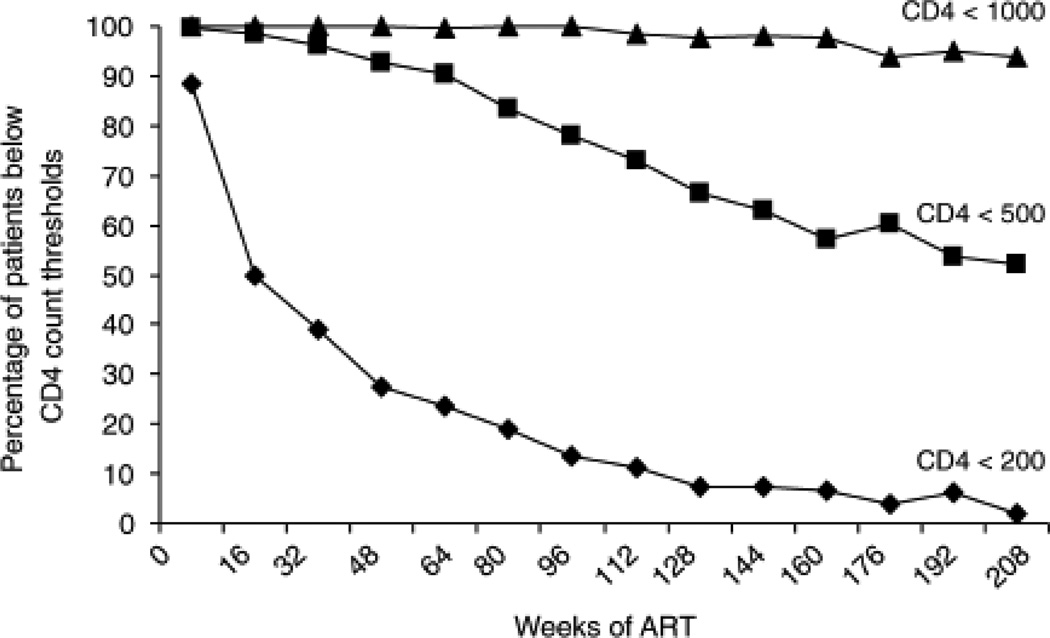
Conclusion: Updated CD4 cell counts were the dominant predictor of TB risk during ART in this low-resource setting. Among those with baseline CD4 cell counts less than 200 cells/microl, the excess adjusted risk of TB during early ART was consistent with 'unmasking' of disease missed at baseline screening. TB incidence rates at CD4 cell counts of 200-500 cells/microl remained high and adjunctive interventions are required. TB prevention would be improved by ART policies that minimized the time patients spend with CD4 cell counts below a threshold of 500 cells/microl.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- Ledergerber B, Egger M, Erard V, Weber R, Hirschel B, Furrer H, et al. AIDS-related opportunistic illnesses occurring after initiation of potent antiretroviral therapy: the Swiss HIV Cohort Study. JAMA. 1999;282:2220–2226. - PubMed
-
- Kirk O, Gatell JM, Mocroft A, Pedersen C, Proenca R, Brettle RP, et al. Infections with Mycobacterium tuberculosis and Mycobacterium avium among HIV-infected patients after the introduction of highly active antiretroviral therapy. EuroSIDA Study Group JD. Am J Respir Crit Care Med. 2000;162:865–872. - PubMed
-
- Girardi E, Antonucci G, Vanacore P, Libanore M, Errante I, Matteelli A, et al. Impact of combination antiretroviral therapy on the risk of tuberculosis among persons with HIV infection. AIDS. 2000;14:1985–1991. Ovid. - PubMed
-
- Jones JL, Hanson DL, Dworkin MS, DeCock KM. HIV-associated tuberculosis in the era of highly active antiretroviral therapy. The Adult/Adolescent Spectrum of HIV Disease Group. Int J Tuberc Lung Dis. 2000;4:1026–1031. - PubMed
-
- Santoro-Lopes G, de Pinho AM, Harrison LH, Schechter M. Reduced risk of tuberculosis among Brazilian patients with advanced human immunodeficiency virus infection treated with highly active antiretroviral therapy. Clin Infect Dis. 2002;34:543–546. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
