

Pseudomonas aeruginosa in a neonatal intensive care unit: molecular epidemiology and infection control measures
- PMID: 19463153
- PMCID: PMC2692859
- DOI: 10.1186/1471-2334-9-70
Pseudomonas aeruginosa in a neonatal intensive care unit: molecular epidemiology and infection control measures
Abstract
Background: Pseudomonas aeruginosa, a non-fermentative, gram-negative rod, is responsible for a wide variety of clinical syndromes in NICU patients, including sepsis, pneumonia, meningitis, diarrhea, conjunctivitis and skin infections. An increased number of infections and colonisations by P. aeruginosa has been observed in the neonatal intensive care unit (NICU) of our university hospital between 2005 and 2007.
Methods: Hand disinfection compliance before and after an educational programme on hand hygiene was evaluated. Identification of microrganisms was performed using conventional methods. Antibiotic susceptibility was evaluated by MIC microdilution. Genotyping was performed by PFGE analysis.
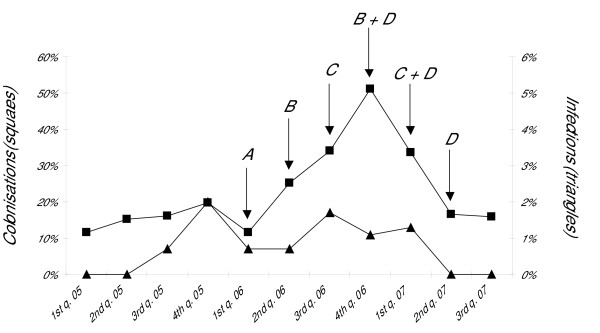
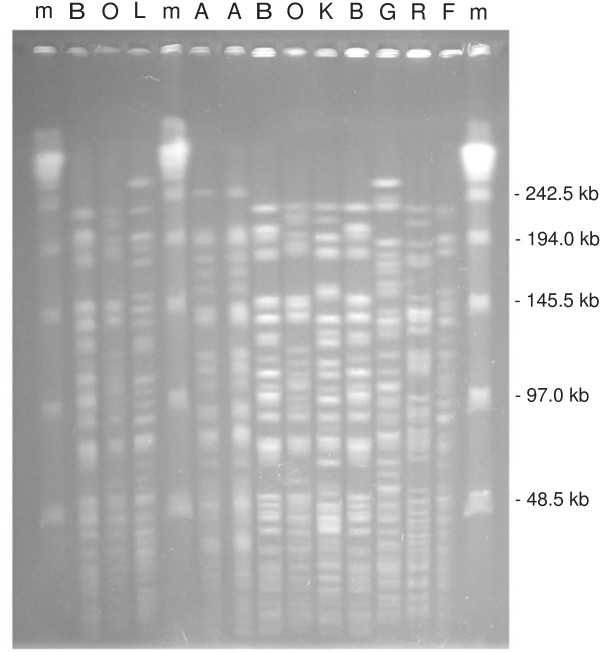
Results: The molecular epidemiology of Pseudomonas aeruginosa in the NICU of the Federico II University hospital (Naples, Italy) and the infection control measures adopted to stop the spreading of P. aeruginosa in the ward were described. From July 2005 to June 2007, P. aeruginosa was isolated from 135 neonates and caused severe infections in 11 of them. Macrorestriction analysis of clinical isolates from 90 neonates identified 20 distinct genotypes, one major PFGE type (A) being isolated from 48 patients and responsible for 4 infections in 4 of them, four other distinct recurrent genotypes being isolated in 6 to 4 patients. Seven environmental strains were isolated from the hand of a nurse and from three sinks on two occasions, two of these showing PFGE profiles A and G identical to two clinical isolates responsible for infection. The successful control of the outbreak was achieved through implementation of active surveillance of healthcare-associated infections in the ward together with environmental microbiological sampling and an intense educational programme on hand disinfection among the staff members.
Conclusion: P. aeruginosa infections in the NICU were caused by the cross-transmission of an epidemic clone in 4 neonates, and by the selection of sporadic clones in 7 others. An infection control programme that included active surveillance and strict adherence to hand disinfection policies was effective in controlling NICU-acquired infections and colonisations caused by P. aeruginosa.
Figures
References
-
- Crivaro V, Bagattini M, Salza MF, Raimondi F, Rossano F, Triassi M, Zarrilli R. Risk factors for extended-spectrum β-lactamase-producing Serratia marcescens and Klebsiella pneumoniae acquisition in a neonatal intensive care unit. J Hosp Infect. 2007;67:135–141. doi: 10.1016/j.jhin.2007.07.026. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
