

Factors related to the selection of surgical versus percutaneous revascularization in diabetic patients with multivessel coronary artery disease in the BARI 2D (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes) trial
- PMID: 19463459
- PMCID: PMC3625397
- DOI: 10.1016/j.jcin.2009.01.009
Factors related to the selection of surgical versus percutaneous revascularization in diabetic patients with multivessel coronary artery disease in the BARI 2D (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes) trial
Abstract
Objectives: We evaluated demographic, clinical, and angiographic factors influencing the selection of coronary artery bypass graft (CABG) surgery versus percutaneous coronary intervention (PCI) in diabetic patients with multivessel coronary artery disease (CAD) in the BARI 2D (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes) trial.
Background: Factors guiding selection of mode of revascularization for patients with diabetes mellitus and multivessel CAD are not clearly defined.
Methods: In the BARI 2D trial, the selected revascularization strategy, CABG or PCI, was based on physician discretion, declared independent of randomization to either immediate or deferred revascularization if clinically warranted. We analyzed factors favoring selection of CABG versus PCI in 1,593 diabetic patients with multivessel CAD enrolled between 2001 and 2005.
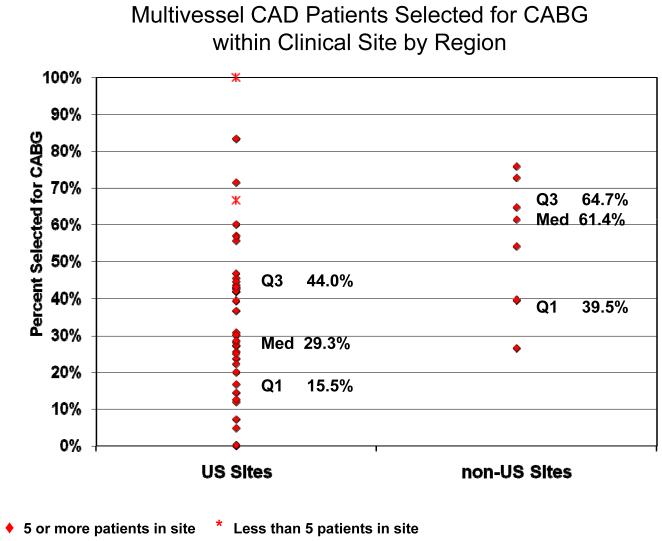
Results: Selection of CABG over PCI was declared in 44% of patients and was driven by angiographic factors including triple vessel disease (odds ratio [OR]: 4.43), left anterior descending stenosis >or=70% (OR: 2.86), proximal left anterior descending stenosis >or=50% (OR: 1.78), total occlusion (OR: 2.35), and multiple class C lesions (OR: 2.06) (all p < 0.005). Nonangiographic predictors of CABG included age >or=65 years (OR: 1.43, p = 0.011) and non-U.S. region (OR: 2.89, p = 0.017). Absence of prior PCI (OR: 0.45, p < 0.001) and the availability of drug-eluting stents conferred a lower probability of choosing CABG (OR: 0.60, p = 0.003).
Conclusions: The majority of diabetic patients with multivessel disease were selected for PCI rather than CABG. Preference for CABG over PCI was largely based on angiographic features related to the extent, location, and nature of CAD, as well as geographic, demographic, and clinical factors. (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes [BARI 2D]; NCT00006305).
Figures


References
-
- Barsness GW, Peterson ED, Ohman EM, et al. Relationship between diabetes mellitus and long-term survival after coronary bypass and angioplasty. Circulation. 1997 Oct 21;96(8):2551–2556. - PubMed
-
- Alderman EL, Corley SD, Fisher LD, et al. Five-year angiographic follow-up of factors associated with progression of coronary artery disease in the Coronary Artery Surgery Study (CASS). CASS Participating Investigators and Staff. J Am Coll Cardiol. 1993;22(4):1141–1154. - PubMed
-
- Thourani VH, Weintraub WS, Stein B, et al. Influence of diabetes mellitus on early and late outcome after coronary artery bypass grafting. Ann Thorac Surg. 1999;67(4):1045–1052. - PubMed
-
- Kip KE, Faxon DP, Detre KM, et al. Coronary angioplasty in diabetic patients. The National Heart, Lung, and Blood Institute Percutaneous Transluminal Coronary Angioplasty Registry. Circulation. 1996 Oct 15;94(8):1818–1825. - PubMed
-
- The Bypass Angioplasty Revascularization Investigation (BARI) Investigators Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996;335(4):217–225. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
