

Does the bronchial circulation contribute to congestion in heart failure?
- PMID: 19464810
- PMCID: PMC2738626
- DOI: 10.1016/j.mehy.2009.03.033
Does the bronchial circulation contribute to congestion in heart failure?
Abstract
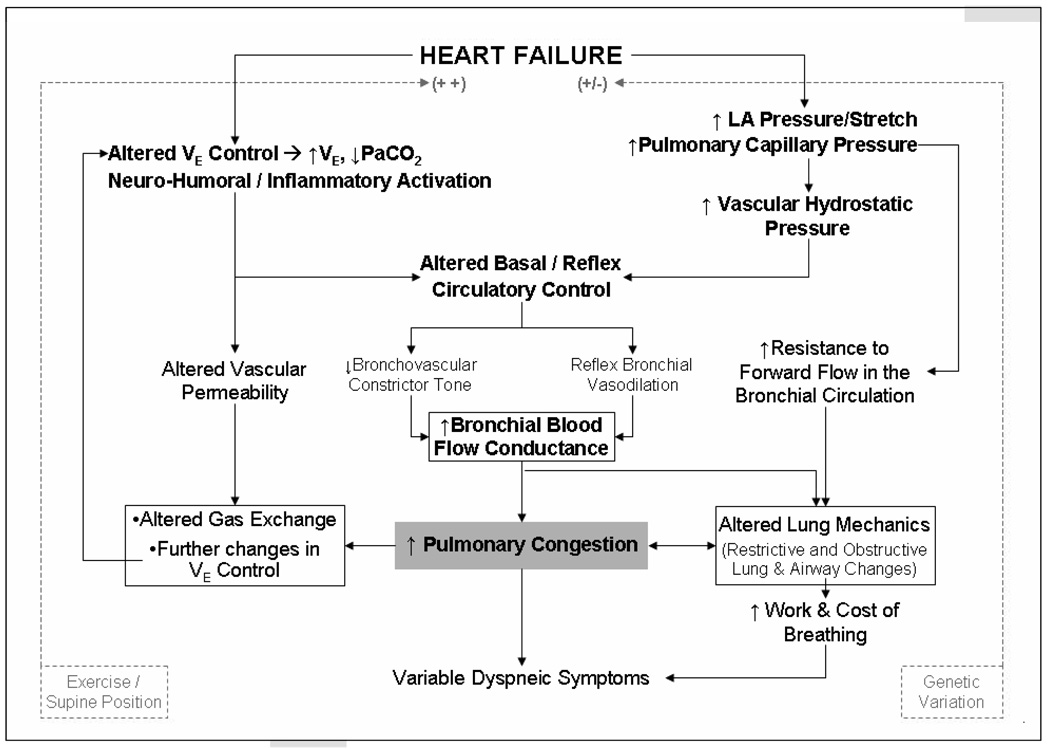
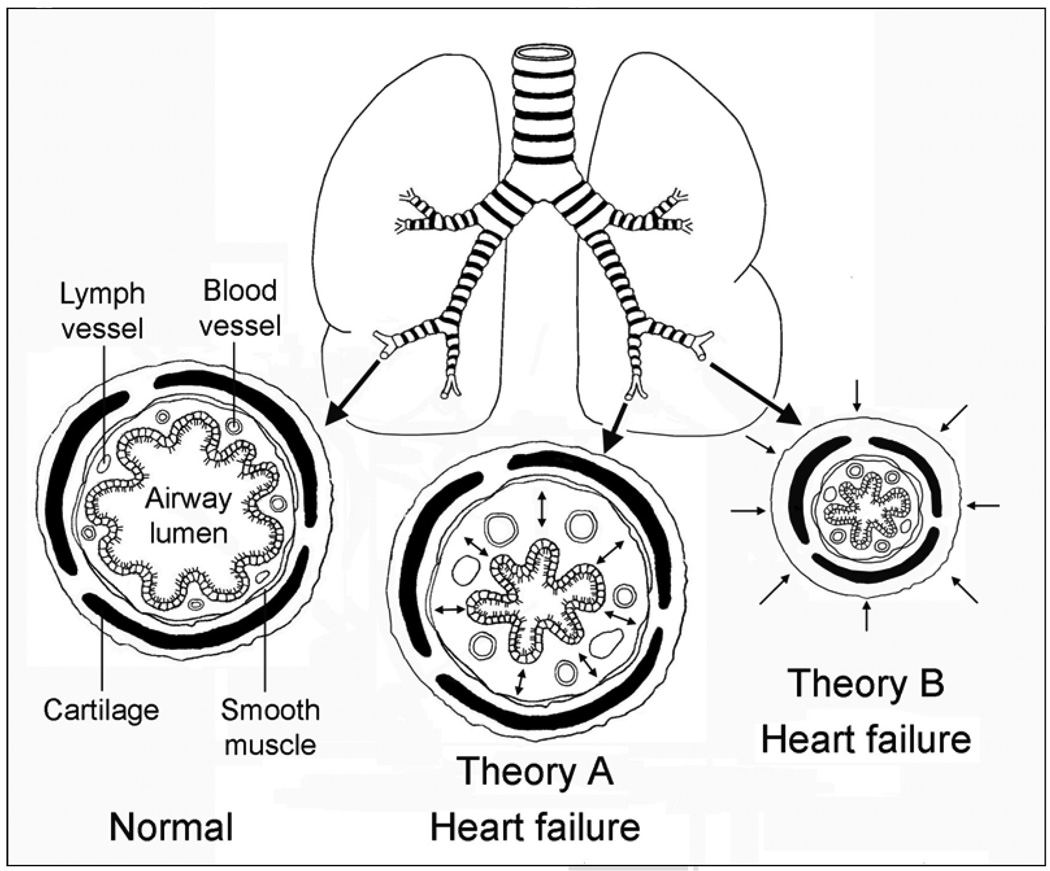
Pulmonary congestion is a hallmark feature of heart failure and is a major reason for hospital admissions in this patient population. Heart failure patients often demonstrate restrictive and obstructive pulmonary function abnormalities; however, the mechanisms of these changes remain controversial. It has been suggested that the bronchial circulation may play an important role in the development of these pulmonary abnormalities and in the symptoms associated with pulmonary congestion. Congestion may occur in the bronchial circulation from either a marked increase in flow or an increase in blood volume but with a reduction in flow due to high cardiac filling pressures and high pulmonary vascular pressures (a stasis like condition). Either may lead to thickened bronchial mucosal and submucosal tissues and reduced airway compliance resulting in airway obstruction and restriction and a lack of airway distensibility. These structural changes may contribute to "cardiac asthma" and dyspnea, characteristic features common in HF patients. Thus the bronchial circulation may be a potential target for therapeutic interventions. The aim of this paper is to review factors governing the control of the bronchial circulation, how bronchial vascular conductance may change with HF and to pose arguments, both supporting and in opposition to the bronchial circulation contributing to congestion and altered pulmonary function in HF. We ultimately hypothesize that the engorgement of the bronchial circulatory bed may play a role in pulmonary function abnormalities that occur in HF patients and contribute to symptoms such as orthopnea and exertional dyspnea.
Figures
Similar articles
-
Influence of bronchial blood flow and conductance on pulmonary function in stable systolic heart failure.Respir Physiol Neurobiol. 2011 Aug 15;177(3):256-64. doi: 10.1016/j.resp.2011.04.020. Epub 2011 Apr 27. Respir Physiol Neurobiol. 2011. PMID: 21545852 Free PMC article.
-
[Vasomotility of the bronchial circulation in cardiac failure].Arch Mal Coeur Vaiss. 1990 Mar;83 Spec No 2:59-62. Arch Mal Coeur Vaiss. 1990. PMID: 2111688 French.
-
Bronchovascular role in pulmonary congestion.Clin Exp Pharmacol Physiol. 2000 Dec;27(12):1045-8. doi: 10.1046/j.1440-1681.2000.03374.x. Clin Exp Pharmacol Physiol. 2000. PMID: 11117228 Review.
-
Cardiac asthma: new insights into an old disease.Expert Rev Respir Med. 2012 Dec;6(6):705-14. doi: 10.1586/ers.12.67. Expert Rev Respir Med. 2012. PMID: 23234454 Review.
-
Systemic to pulmonary bronchial blood flow in heart failure.Chest. 1995 May;107(5):1247-52. doi: 10.1378/chest.107.5.1247. Chest. 1995. PMID: 7750314
Cited by
-
Influence of lung volume, fluid and capillary recruitment during positional changes and exercise on thoracic impedance in heart failure.Respir Physiol Neurobiol. 2014 Oct 1;202:75-81. doi: 10.1016/j.resp.2014.08.001. Epub 2014 Aug 14. Respir Physiol Neurobiol. 2014. PMID: 25128641 Free PMC article.
-
Impact of chronic systolic heart failure on lung structure-function relationships in large airways.Physiol Rep. 2016 Jul;4(13):e12867. doi: 10.14814/phy2.12867. Physiol Rep. 2016. PMID: 27418546 Free PMC article.
-
Effect of supine posture on airway blood flow and pulmonary function in stable heart failure.Respir Physiol Neurobiol. 2011 Sep 15;178(2):269-74. doi: 10.1016/j.resp.2011.06.021. Epub 2011 Jun 30. Respir Physiol Neurobiol. 2011. PMID: 21741500 Free PMC article.
-
Pulmonary Limitations in Heart Failure.Clin Chest Med. 2019 Jun;40(2):439-448. doi: 10.1016/j.ccm.2019.02.010. Clin Chest Med. 2019. PMID: 31078220 Free PMC article. Review.
-
Influence of bronchial blood flow and conductance on pulmonary function in stable systolic heart failure.Respir Physiol Neurobiol. 2011 Aug 15;177(3):256-64. doi: 10.1016/j.resp.2011.04.020. Epub 2011 Apr 27. Respir Physiol Neurobiol. 2011. PMID: 21545852 Free PMC article.
References
-
- Gheorghiade M, Shin DD, Thomas TO, Brandimarte F, Fonarow GC, Abraham WT. Congestion is an important diagnostic and therapeutic target in heart failure. Rev Cardiovasc Med. 2006;7 Suppl 1:S12–S24. - PubMed
-
- Gheorghiade M, Filippatos G, De Luca L, Burnett J. Congestion in acute heart failure syndromes: an essential target of evaluation and treatment. Am J Med. 2006;119:S3–S10. - PubMed
-
- Gehlbach BK, Geppert E. The pulmonary manifestations of left heart failure. Chest. 2004;125:669–682. - PubMed
-
- Faggiano P. Abnormalities of pulmonary function in congestive heart failure. International journal of cardiology. 1994;44:1–8. - PubMed
-
- Deffebach ME, Charan NB, Lakshminarayan S, Butler J. The bronchial circulation. Small, but a vital attribute of the lung. Am Rev Respir Dis. 1987;135:463–481. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
