

Effect of fenofibrate on amputation events in people with type 2 diabetes mellitus (FIELD study): a prespecified analysis of a randomised controlled trial
- PMID: 19465233
- PMCID: PMC2687887
- DOI: 10.1016/S0140-6736(09)60698-X
Effect of fenofibrate on amputation events in people with type 2 diabetes mellitus (FIELD study): a prespecified analysis of a randomised controlled trial
Abstract
Background: Amputations in people with type 2 diabetes mellitus substantially impair their quality of life and impose high costs on health-care systems. Our aim was to assess the effect of fenofibrate on amputation events in a large cohort of patients with type 2 diabetes.
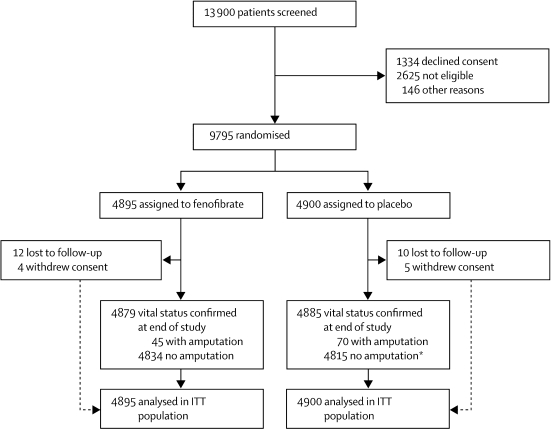
Methods: In the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study, 9795 patients aged 50-75 years with type 2 diabetes were randomly assigned by computer-generated randomisation sequence to receive fenofibrate 200 mg per day (n=4895) or matching placebo (n=4900) for 5 years' duration. Information about non-traumatic amputation-a prespecified tertiary endpoint of the study-was routinely gathered. Clinicians who were masked to treatment allocation adjudicated amputations as minor or major (below or above the ankle, respectively). Amputations were also classified on the basis of whether or not large-vessel disease was present in the limb, to distinguish those related to large-artery atherosclerosis from those predominantly related to microvascular disease. Analysis was by intention to treat (ITT). The FIELD study is registered as an International Standard Randomised Controlled Trial, number ISRCTN64783481.
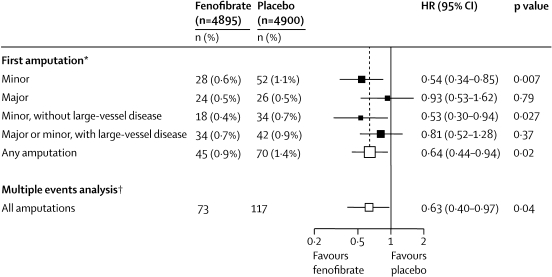
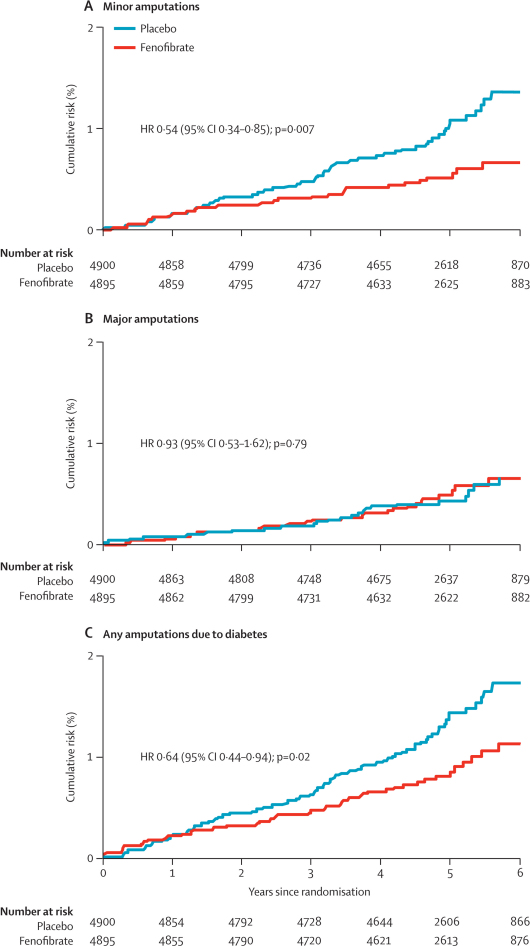
Findings: All 9795 patients were included in the ITT population. 115 patients had one or more non-traumatic lower-limb amputations due to diabetes. Previous cardiovascular disease, microvascular disease, previous non-traumatic amputation or skin ulcer, smoking, and longer duration of diabetes were more frequent in patients who had amputations during the trial than in those who had other cardiovascular events or in those who had neither event (all p<0.001 for three-way comparison). Mean lipid concentrations differed between patients who had on-study amputations and those who had other cardiovascular events or neither event, but by no more than 0.2 mmol/L. The risks of first amputation (45 vs 70 events; hazard ratio [HR] 0.64, 95% CI 0.44-0.94; p=0.02) and minor amputation events without known large-vessel disease (18 vs 34 events; 0.53, 0.30-0.94; p=0.027) were lower for patients assigned to fenofibrate than for patients assigned to placebo, with no difference between groups in risk of major amputations (24 vs 26 events; 0.93, 0.53-1.62; p=0.79).
Interpretation: Classic markers of macrovascular and microvascular risk were associated with lower extremity amputations in patients with type 2 diabetes. Treatment with fenofibrate was associated with a lower risk of amputations, particularly minor amputations without known large-vessel disease, probably through non-lipid mechanisms. These findings could lead to a change in standard treatment for the prevention of diabetes-related lower-limb amputations.
Funding: Laboratoires Fournier SA (now part of Solvay Pharmaceuticals) and National Health and Medical Research Council of Australia.
Figures
Comment in
-
Fenofibrate and risk of minor amputations in diabetes.Lancet. 2009 May 23;373(9677):1740-1. doi: 10.1016/S0140-6736(09)60959-4. Lancet. 2009. PMID: 19465214 No abstract available.
References
-
- Bild DE, Selby JV, Sinnock P. Low-extremity amputation in people with diabetes. Epidemiology and prevention. Diabetes Care. 1980;12:24–31. - PubMed
-
- American Diabetes Association Economic costs of diabetes in the US in 2002. Diabetes Care. 2003;26:917–932. - PubMed
-
- Gordois A, Scuffham P, Shearer A. The health care cost of diabetic peripheral neuropathy in the US. Diabetes Care. 2003;26:1790–1795. - PubMed
-
- The FIELD study investigators Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849–1861. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
