Surgical approach in patients with T4 bladder cancer as primary treatment: Disaster or option with improved quality of life
- PMID: 19468367
- PMCID: PMC2684222
- DOI: 10.4103/0970-1591.38610
Surgical approach in patients with T4 bladder cancer as primary treatment: Disaster or option with improved quality of life
Abstract
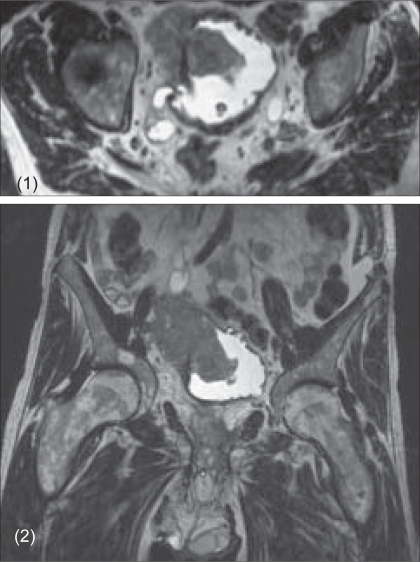
Objectives: Whereas local control is often insufficient in conservative management of T4 bladder cancer, neoadjuvant chemotherapy delays definite treatment, which could result in increased therapy-associated morbidity and mortality during the course of the disease. Primary cystectomy has been reported to be associated with a high complication rate and unsatisfactory clinical efficacy. Herein, we report postoperative outcome in 21 T4 bladder cancer patients subjected to primary cystectomy.
Materials and methods: Twenty-one patients underwent radical cystectomy for T4 (T4a/b: 14 and seven cases, respectively) bladder cancer. At the time of surgery, eight patients had regional lymph node metastases (N2: 6; N3: 2). The average age was 64 (52-77) years (>/=70 years: n = 7). The postoperative follow-up was 13 (1-36) months for the whole group.
Results: Mean duration of postoperative hospitalization was 19 (11-50) days. Whereas 10 patients received no intra - or postoperative blood transfusions, an average number of 3 (1-7) blood units were administered in the remaining cases. The mean postoperative hemoglobin value of patients not receiving any blood transfusions was 10 (8.5 - 11.4) g/dl. Major therapy-associated complications were paresthesia affecting the lower extremities (n = 3) as well as insignificant pulmonary embolism, enterocutaneous fistulation and acute renal failure in one patient, respectively. At the time of data evaluation, 11 patients were still alive after a follow-up of 20 (6-36) months. Four patients >/=70 years at the time of cystectomy were still alive 11, 11, 22 and 31 months following surgery, respectively.
Conclusion: Primary cystectomy for T4 bladder cancer is a technically feasible approach that is associated with a tolerable therapy-related morbidity/mortality. Additionally, a satisfactory clinical outcome is observed even in a substantial number of elderly patients.
Keywords: Bladder cancer; cystectomy; survival; treatment.
Conflict of interest statement
Figures
Similar articles
-
The rationale for radical cystectomy as primary therapy for T4 bladder cancer.World J Urol. 2007 Aug;25(4):401-5. doi: 10.1007/s00345-007-0172-9. Epub 2007 May 25. World J Urol. 2007. PMID: 17525849
-
[Results of radical cystectomy for management of invasive bladder cancer with special reference to prognostic factors and quality of life depending on the type of urinary diversion].Ann Acad Med Stetin. 2000;46:217-29. Ann Acad Med Stetin. 2000. PMID: 11712306 Polish.
-
A study of the morbidity, mortality and long-term survival following radical cystectomy and radical radiotherapy in the treatment of invasive bladder cancer in Yorkshire.Eur Urol. 2003 Mar;43(3):246-57. doi: 10.1016/s0302-2838(02)00581-x. Eur Urol. 2003. PMID: 12600427
-
[Analysis of 34 cases of infiltrating carcinoma of the bladder treated exclusively with partial cystectomy (part 1)].Arch Esp Urol. 1996 May;49(4):349-64. Arch Esp Urol. 1996. PMID: 8754191 Review. Spanish.
-
[Neoadjuvant and adjuvant chemotherapy of bladder cancer].Gan To Kagaku Ryoho. 1994 Oct;21 Suppl 3:362-9. Gan To Kagaku Ryoho. 1994. PMID: 7986116 Review. Japanese.
Cited by
-
Laparoscopic radical cystectomy: initial experience using the single-incision triangulated umbilical surgery (SITUS) technique.World J Urol. 2012 Oct;30(5):619-24. doi: 10.1007/s00345-012-0909-y. Epub 2012 Jul 21. World J Urol. 2012. PMID: 22820621 Clinical Trial.
-
Clinicopathologic characteristics and overall survival in patients with bladder cancer involving the gastrointestinal tract.Virchows Arch. 2013 Dec;463(6):811-8. doi: 10.1007/s00428-013-1479-0. Epub 2013 Oct 4. Virchows Arch. 2013. PMID: 24092260
-
Radical cystectomy for clinical T4b urothelial carcinoma: An Ontario, single-center experience.Can Urol Assoc J. 2022 May;16(5):E274-E277. doi: 10.5489/cuaj.7277. Can Urol Assoc J. 2022. PMID: 34941484 Free PMC article.
-
Open versus Robot-Assisted Radical Cystectomy for the Treatment of pT4a Bladder Cancer: Comparison of Perioperative Outcomes.Cancers (Basel). 2024 Mar 28;16(7):1329. doi: 10.3390/cancers16071329. Cancers (Basel). 2024. PMID: 38611006 Free PMC article.
References
-
- Skinner DG, Stein JP, Lieskovsky G, Skinner EC, Boyd SD, Figueroa A, et al. 25-year experience in the management of invasive bladder cancer by radical cystectomy. Eur Urol. 1998;33:25–6. - PubMed
-
- Figueroa AJ, Stein JP, Dickinson M, Skinner EC, Thangathurai D, Mikhail MS, et al. Radical cystectomy for elderly patients with bladder carcinoma: An updated experience with 404 patients. Cancer. 1998;83:141–7. - PubMed
-
- Zebic N, Weinknecht S, Kroepfl D. Radical cystectomy in patients aged > or = 75 years: An updated review of patients treated with curative and palliative intent. BJU Int. 2005;95:1211–4. - PubMed
-
- Rödel C, Grabenbauer GG, Kühn R, Papadopoulos T, Dunst J, Meyer M, et al. Combined-modality treatment and selective organ preservation in invasive bladder cancer: Long-term results. J Clin Oncol. 2002;20:3061–71. - PubMed
-
- Dunst J, Diestelhorst A, Kühn R, Müller AC, Scholz HJ, Fornara P. Organ-sparing treatment in muscle-invasive bladder cancer. Strahlenther Onkol. 2005;181:632–7. - PubMed