

Trigger finger: etiology, evaluation, and treatment
- PMID: 19468879
- PMCID: PMC2684207
- DOI: 10.1007/s12178-007-9012-1
Trigger finger: etiology, evaluation, and treatment
Abstract
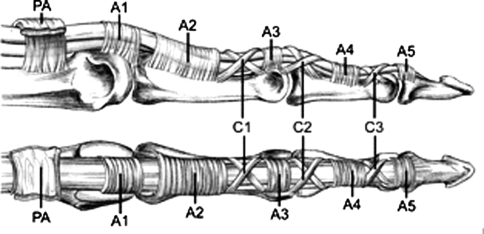
Trigger finger is a common finger aliment, thought to be caused by inflammation and subsequent narrowing of the A1 pulley, which causes pain, clicking, catching, and loss of motion of the affected finger. Although it can occur in anyone, it is seen more frequently in the diabetic population and in women, typically in the fifth to sixth decade of life. The diagnosis is usually fairly straightforward, as most patients complain of clicking or locking of the finger, but other pathological processes such as fracture, tumor, or other traumatic soft tissue injuries must be excluded. Treatment modalities, including splinting, corticosteroid injection, or surgical release, are very effective and are tailored to the severity and duration of symptoms.
Figures

References
-
- Notta A. Recherches sur une affection particuliere des gaines tendineuses de la main. Arch Gen Med. 1850;24:142.
-
- Carlson CS, Jr, Curtis RM. Steroid injection for flexor tenosynovitis. J Hand Surg [Am] 1984;9:286–7. - PubMed
-
- Rhoades CE, Gelberman RH, Manjarris JF. Stenosing tenosynovitis of the fingers and thumb. Results of a prospective trial of steroid injection and splinting. Clin Orthop Relat Res. 1984;190:236–8. - PubMed
-
- Fahey JJ, Bollinger JA. Trigger-finger in adults and children. J Bone Joint Surg Am. 1954;36:1200–18. - PubMed
LinkOut - more resources
Full Text Sources
Medical
