

Proliferative glomerulonephritis with monoclonal IgG deposits
- PMID: 19470674
- PMCID: PMC2736767
- DOI: 10.1681/ASN.2009010110
Proliferative glomerulonephritis with monoclonal IgG deposits
Abstract
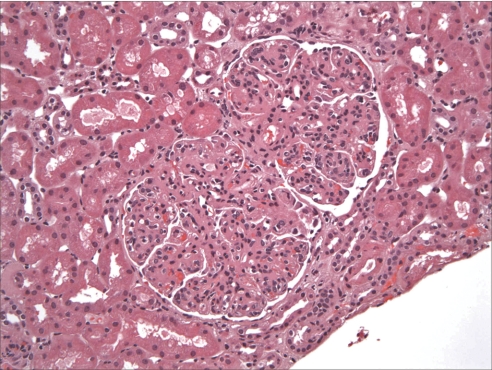
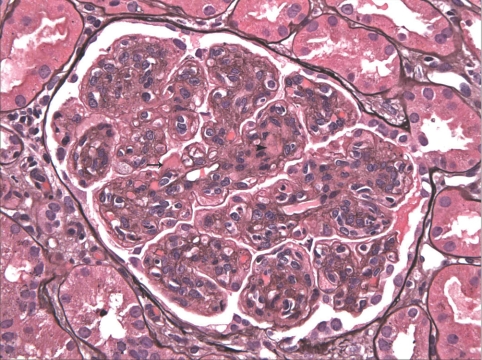
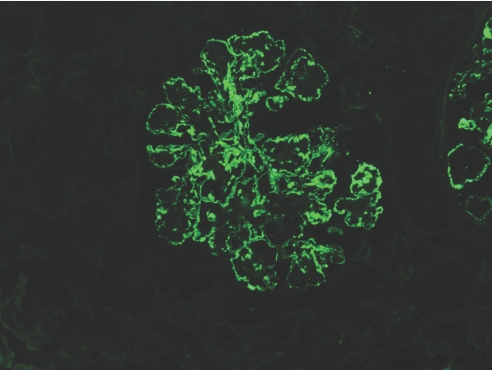
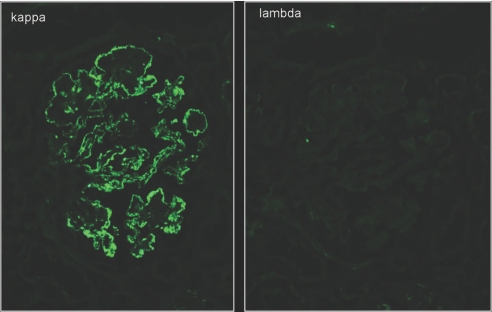
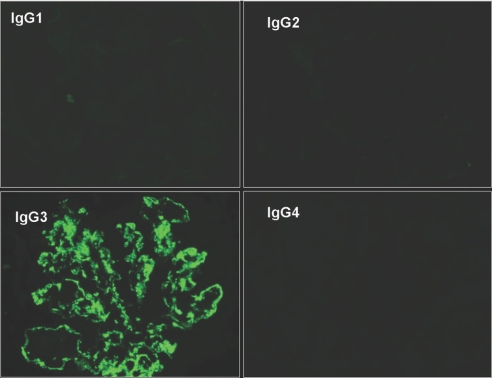
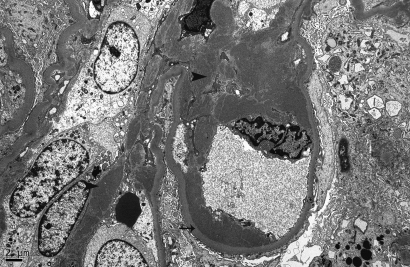
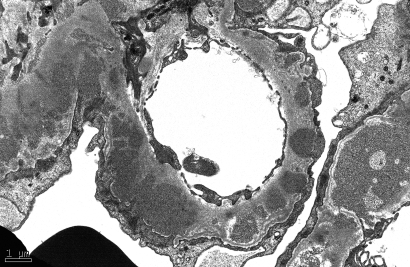
Dysproteinemias that result in monoclonal glomerular deposits of IgG are relatively uncommon. Here, we report the largest series of proliferative glomerulonephritis with monoclonal IgG deposits, a form of renal involvement by monoclonal gammopathy that mimics immune-complex glomerulonephritis. We retrospectively identified 37 patients, most of whom were white (81%), female (62%), or older than 50 yr (65%). At presentation, 49% had nephrotic syndrome, 68% had renal insufficiency, and 77% had hematuria. In 30% of the patients, we identified a monoclonal serum protein with the same heavy- and light-chain isotypes as the glomerular deposits (mostly IgG1 or IgG2), but only one patient had myeloma. Histologic patterns were predominantly membranoproliferative (57%) or endocapillary proliferative (35%) with membranous features. Electron microscopy revealed granular, nonorganized deposits, and immunofluorescence demonstrated glomerular deposits that stained for a single light-chain isotype and a single heavy-chain subtype, most commonly IgG3kappa (53%). During an average of 30.3 mo of follow-up for 32 patients with available data, 38% had complete or partial recovery, 38% had persistent renal dysfunction, and 22% progressed to ESRD. Correlates of ESRD on univariate analysis were higher creatinine at biopsy, percentage of glomerulosclerosis, and degree of interstitial fibrosis but not immunomodulatory treatment or presence of a monoclonal spike. On multivariate analysis, higher percentage of glomerulosclerosis was the only independent predictor of ESRD. Only one patient lacking a monoclonal spike at presentation subsequently developed a monoclonal spike and no patient with a monoclonal spike at presentation subsequently developed a hematologic malignancy. We conclude that proliferative glomerulonephritis with monoclonal IgG deposits does not seem to be a precursor of myeloma in the vast majority of patients.
Figures
References
-
- Lin J, Markowitz GS, Valeri AM, Kambham N, Sherman WH, Appel GB, D'Agati VD:Renal monoclonal immunoglobulin deposition disease: The disease spectrum. J Am Soc Nephrol 12: 1482–1492, 2001 - PubMed
-
- Nasr SH, Markowitz GS, Reddy BS, Maesaka J, Swidler MA, D'Agati VD:Dysproteinemia, proteinuria, and glomerulonephritis. Kidney Int 69: 772–775, 2006 - PubMed
-
- Rosenstock JL, Markowitz GS, Valeri AM, Sacchi G, Appel GB, D'Agati VD:Fibrillary and immunotactoid glomerulonephritis: Distinct entities with different clinical and pathologic features. Kidney Int 63: 1450–1461, 2003 - PubMed
-
- Nasr SH, Colvin R, Markowitz GS:IgG1 lambda light and heavy chain renal amyloidosis. Kidney Int 70: 7, 2006 - PubMed
-
- Nasr SH, Markowitz GS, Stokes MB, Seshan SV, Valderrama E, Appel GB, Aucouturier P, D'Agati VD:Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis. Kidney Int 65: 85–96, 2004 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
