

Daclizumab versus antithymocyte globulin in high-immunological-risk renal transplant recipients
- PMID: 19470677
- PMCID: PMC2689909
- DOI: 10.1681/ASN.2008101037
Daclizumab versus antithymocyte globulin in high-immunological-risk renal transplant recipients
Abstract
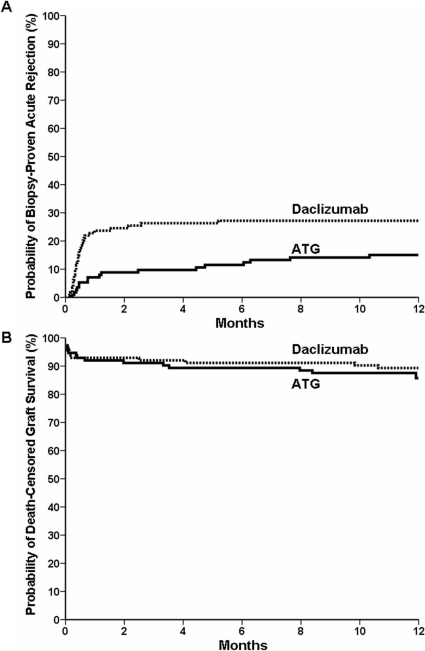
Nondepleting anti-CD25 monoclonal antibodies (daclizumab) and depleting polyclonal antithymocyte globulin (Thymoglobulin) both prevent acute rejection, but these therapies have not been directly compared in a high-risk, HLA-sensitized renal transplant population. We randomly assigned 227 patients, who were about to receive a kidney graft from a deceased donor, to either Thymoglobulin or daclizumab if they met one of the following risk factors: current panel reactive antibodies (PRA) >30%; peak PRA >50%; loss of a first kidney graft from rejection within 2 yr of transplantation; or two or three previous grafts. Maintenance immunosuppression comprised tacrolimus, mycophenolate mofetil, and steroids. Compared with the daclizumab group, patients treated with Thymoglobulin had a lower incidence of both biopsy-proven acute rejection (15.0% versus 27.2%; P = 0.016) and steroid-resistant rejection (2.7% versus 14.9%; P = 0.002) at one year. One-year graft and patient survival rates were similar between the two groups. In a comparison of rejectors and nonrejectors, overall graft survival was significantly higher in the rejection-free group (87.2% versus 75.0%; P = 0.037). In conclusion, among high-immunological-risk renal transplant recipients, Thymoglobulin is superior to daclizumab for the prevention of biopsy-proven acute rejection, but there is no significant benefit to one-year graft or patient survival.
Figures

Comment in
-
Anti-IL-2 receptor antibodies versus anti-thymocyte globulin for induction therapy in kidney transplantation.J Am Soc Nephrol. 2009 Jun;20(6):1170-1. doi: 10.1681/ASN.2009040389. Epub 2009 May 21. J Am Soc Nephrol. 2009. PMID: 19470672 No abstract available.
References
-
- Wissing KM, Fomegne G, Broeders N, Ghisdal L, Hoang AD, Mikhalski D, Donckier V, Vereerstraeten P, Abramowicz D: HLA mismatches remain risk factors for acute kidney allograft rejection in patients receiving quadruple immunosuppression with anti-interleukin-2 receptor antibodies. Transplantation 85: 411–416, 2008 - PubMed
-
- Andreoni KA, Brayman KL, Guidinger MK, Sommers CM, Sung RS: Kidney and pancreas transplantation in the United States, 1996–2005. Am J Transplant 7: 1359–1375, 2007 - PubMed
-
- Webster AC, Playford EG, Higgins G, Chapman JR, Craig JC: Interleukin 2 receptor antagonists for renal transplant recipients: A meta-analysis of randomized trials. Transplantation 77: 166–176, 2004 - PubMed
-
- Vincenti F, de Andrés A, Becker T, Choukroun G, Cole E, Gonzalez-Posada JM, Kumar MA, Moore R, Nadalin S, Nashan B, Rostaing L, Saito K, Yoshimura N: Interleukin-2 receptor antagonist induction in modern immunosuppression regimens for renal transplant recipients. Transpl Int 19: 446–457, 2006 - PubMed
-
- Patlolla V, Zhong X, Reed GW, Mandelbrot DA: Efficacy of anti-IL-2 receptor antibodies compared to no induction and to antilymphocyte antibodies in renal transplantation. Am J Transplant 7: 1832–1842, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
