

Hospital factors and racial disparities in mortality after surgery for breast and colon cancer
- PMID: 19470926
- PMCID: PMC2734396
- DOI: 10.1200/JCO.2008.20.8546
Hospital factors and racial disparities in mortality after surgery for breast and colon cancer
Abstract
Purpose: Black patients have worse prognoses than whites with breast or colorectal cancer. Mechanisms underlying such disparities have not been fully explored. We examined the role of hospital factors in racial differences in late mortality after surgery for breast or colon cancer.
Methods: Patients undergoing surgery after new diagnosis of breast or colon cancer were identified using the Surveillance Epidemiology and End Results-Medicare linked database (1995 to 2005). The main outcome measure was mortality at 5 years. Proportional hazards models were used to assess relationships between race and late mortality, accounting for patient factors, socioeconomic measures, and hospital factors. Fixed and random effects models were used to account for quality differences across hospitals.
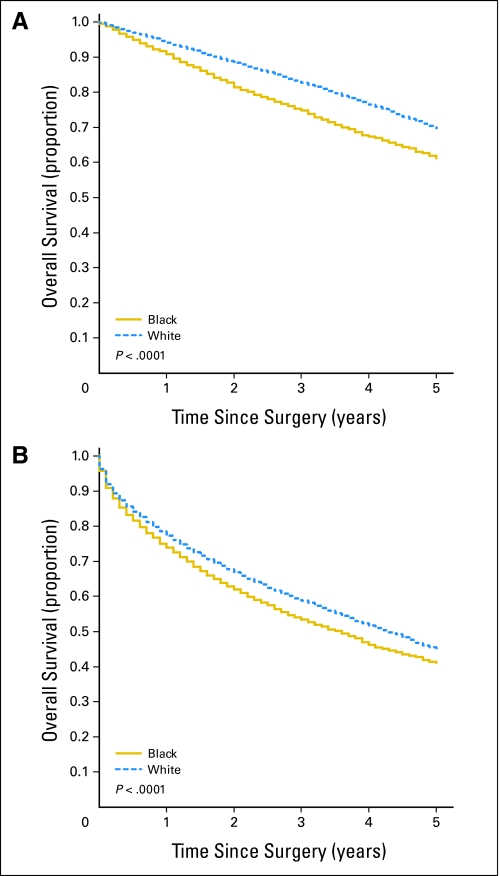
Results: Black patients, compared with white patients, had lower 5-year overall survival rates after surgery for breast (62.1% v 70.4%, respectively; P < .001) and colon cancer (41.3% v 45.4%, respectively; P < .001). After controlling for age, comorbidity, and stage, black race remained an independent predictor of mortality for breast (adjusted hazard ratio [HR] = 1.25; 95% CI, 1.16 to 1.34) and colon cancer (adjusted HR = 1.13; 95% CI, 1.07 to 1.19). After risk adjustment, hospital factors explained 36% and 54% of the excess mortality for black patients with breast cancer and colon cancer, respectively. Hospitals with large minority populations had higher late mortality rates independent of race.
Conclusion: Hospital factors, including quality, are important mediators of the association between race and mortality for breast and colon cancer. Hospital-level quality improvement should be a major component of efforts to reduce disparities in cancer outcomes.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Findings that hospital factors are surrogate for disparities are misleading.J Clin Oncol. 2010 Feb 1;28(4):e56; author reply e57. doi: 10.1200/JCO.2009.26.1107. Epub 2009 Dec 14. J Clin Oncol. 2010. PMID: 20008617 No abstract available.
References
-
- Ward E, Jemal A, Cokkinides V, et al. Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin. 2004;54:78–93. - PubMed
-
- Lund MJ, Brawley OP, Ward KC, et al. Parity and disparity in first course treatment of invasive breast cancer. Breast Cancer Res Treat. 2008;109:545–557. - PubMed
-
- Newman LA, Griffith KA, Jatoi I, et al. Meta-analysis of survival in African American and white American patients with breast cancer: Ethnicity compared with socioeconomic status. J Clin Oncol. 2006;24:1342–1349. - PubMed
-
- Cunningham JE, Butler WM. Racial disparities in female breast cancer in South Carolina: Clinical evidence for a biological basis. Breast Cancer Res Treat. 2004;88:161–176. - PubMed
-
- Schatzkin A. Variation in inpatient racial composition among acute-care hospitals in New York State. Soc Sci Med. 1985;20:371–379. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
