

Optimized antidepressant therapy and pain self-management in primary care patients with depression and musculoskeletal pain: a randomized controlled trial
- PMID: 19470987
- PMCID: PMC2884224
- DOI: 10.1001/jama.2009.723
Optimized antidepressant therapy and pain self-management in primary care patients with depression and musculoskeletal pain: a randomized controlled trial
Abstract
Context: Pain and depression are the most common physical and psychological symptoms in primary care, respectively. Moreover, they co-occur 30% to 50% of the time and have adverse effects on quality of life, disability, and health care costs.
Objective: To determine if a combined pharmacological and behavioral intervention improves both depression and pain in primary care patients with musculoskeletal pain and comorbid depression.
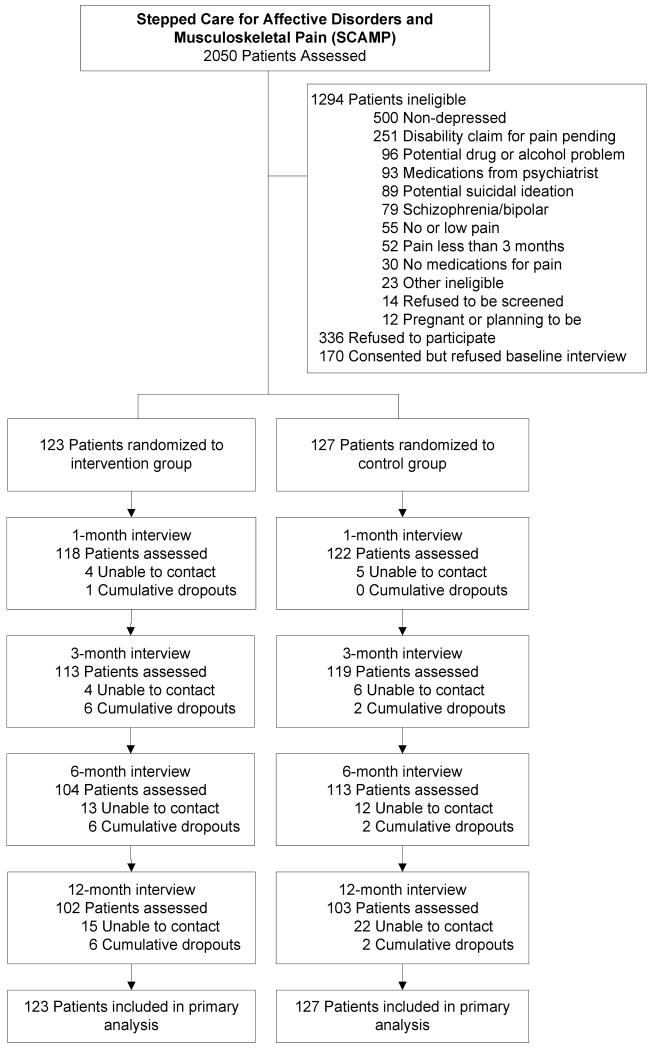
Design, setting, and patients: Randomized controlled trial (Stepped Care for Affective Disorders and Musculoskeletal Pain [SCAMP]) conducted at 6 community-based clinics and 5 Veterans Affairs general medicine clinics in Indianapolis, Indiana. Recruitment occurred from January 2005 to June 2007 and follow-up concluded in June 2008. The 250 patients had low back, hip, or knee pain for 3 months or longer and at least moderate depression severity (Patient Health Questionnaire 9 score > or = 10).
Intervention: Patients were randomly assigned to the intervention (n = 123) or to usual care (n = 127). The intervention consisted of 12 weeks of optimized antidepressant therapy (step 1) followed by 6 sessions of a pain self-management program over 12 weeks (step 2), and a continuation phase of therapy for 6 months (step 3).
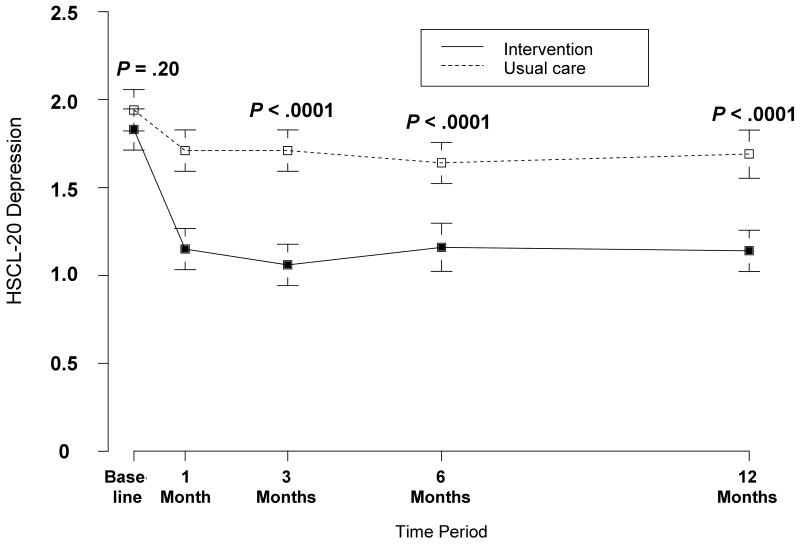
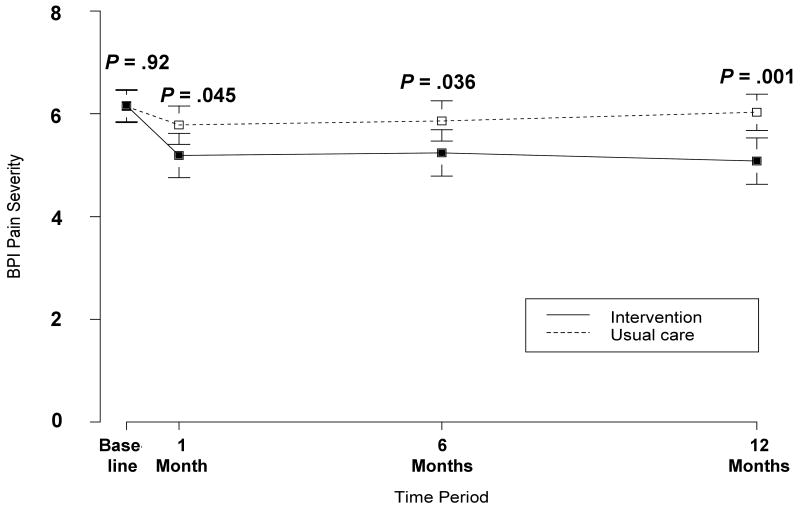
Main outcome measures: Depression (20-item Hopkins Symptom Checklist), pain severity and interference (Brief Pain Inventory), and global improvement in pain at 12 months.
Results: At 12 months, 46 of the 123 intervention patients (37.4%) had a 50% or greater reduction in depression severity from baseline compared with 21 of 127 usual care patients (16.5%) (relative risk [RR], 2.3; 95% confidence interval [CI], 1.5-3.2), corresponding to a much lower number of patients with major depression (50 [40.7%] vs 87 [68.5%], respectively; RR, 0.6 [95% CI, 0.4-0.8]). Also, a clinically significant (> or = 30%) reduction in pain was much more likely in intervention patients (51 intervention patients [41.5%] vs 22 usual care patients [17.3%]; RR, 2.4 [95% CI, 1.6-3.2]), as was global improvement in pain (58 [47.2%] vs 16 [12.6%], respectively; RR, 3.7 [95% CI, 2.3-6.1]). More intervention patients also experienced benefits in terms of the primary outcome, which was a combined improvement in both depression and pain (32 intervention patients [26.0%] vs 10 usual care patients [7.9%]; RR, 3.3 [95% CI, 1.8-5.4]).
Conclusion: Optimized antidepressant therapy followed by a pain self-management program resulted in substantial improvement in depression as well as moderate reductions in pain severity and disability.
Trial registration: clinicaltrials.gov Identifier: NCT00118430.
Figures
Comment in
-
Compined pain self-management and antidepressant therapy are effective in patients with chronic musculoskeletal pain with depression.Aust J Physiother. 2009;55(3):208. doi: 10.1016/s0004-9514(09)70084-4. Aust J Physiother. 2009. PMID: 19736674 No abstract available.
-
Antidepressants combined with self-management of pain improves outcomes in people with comorbid pain and depression.Evid Based Ment Health. 2010 Feb;13(1):13. doi: 10.1136/ebmh.13.1.13. Evid Based Ment Health. 2010. PMID: 20164510 No abstract available.
References
-
- Spitzer RL, Kroenke K, Linzer M, et al. Health-related quality of life in primary care patients with mental disorders: results from the PRIME-MD 1000 study. JAMA. 1995;274:1511–1517. - PubMed
-
- Schappert SM. National Ambulatory Medical Care Survey: 1989 summary National Center for Health Statistics. Vital Health Stat. 1992;13(110) - PubMed
-
- Sternbach RA. Survey of Pain in the United States: The Nuprin Pain Report. Clin J Pain. 1986;2:49–53. - PubMed
-
- Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163:2433–2445. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
