

Features at diagnosis of 324 patients with acromegaly did not change from 1981 to 2006: acromegaly remains under-recognized and under-diagnosed
- PMID: 19473180
- PMCID: PMC2866138
- DOI: 10.1111/j.1365-2265.2009.03626.x
Features at diagnosis of 324 patients with acromegaly did not change from 1981 to 2006: acromegaly remains under-recognized and under-diagnosed
Abstract
Background: Traditionally, acromegaly evaded diagnosis until in its clinically obvious later stages when treatment is more difficult. Over the last 25 years diagnostic tests have improved, but whether clinical disease detection also improved was unknown, so we tested if disease severity at diagnosis had changed from 1981 to 2006.
Methods: Data on 324 consecutive acromegaly patients presenting from 1981 to 2006 at two New York City hospitals were collected by retrospective review (n = 324) and by interview (n = 200). The main complaint, acromegaly associated comorbidities, signs, symptoms, healthcare providers visited, preoperative GH and IGF-I levels and pituitary tumour size at diagnosis were compared in patients presenting in the earlier vs. later halves of the time period.
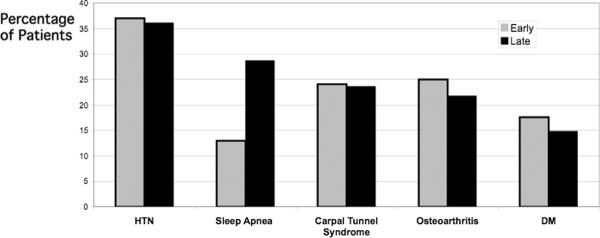
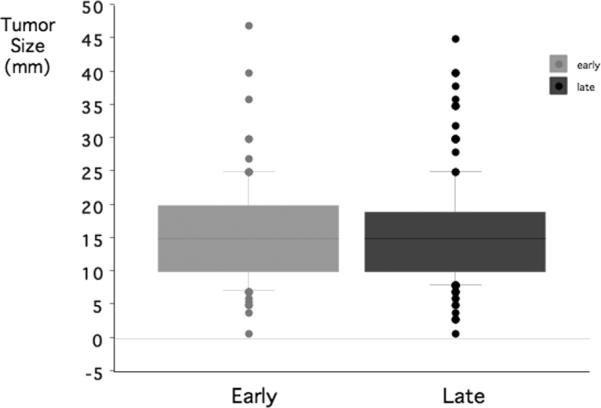
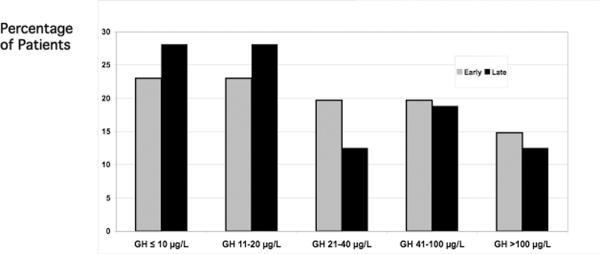
Results: Times from symptom onset to diagnosis were 5.9 year (early) vs. 5.2 year (late; P = NS). At diagnosis, 96% of early and late groups had facial feature changes and/or hand/foot enlargement. Comorbidities included hypertension 37% (early) vs. 36% (late), carpal tunnel syndrome (24%vs. 24%), sleep apnoea (13%vs. 29%; P < 0.01), osteoarthritis (25%vs. 23%) and diabetes mellitus (18%vs. 15%); each patient had 1.2 (early) vs. 1.3 (late; P = 0.53) comorbidities. Groups were similar in signs, symptoms, tumour size, GH and IGF-I.
Conclusions: Clinical, biochemical and tumour size characteristics at diagnosis of acromegaly patients were unchanged from 1981 to 2006. Most patients still have marked manifestations of acromegaly at diagnosis, suggesting that acromegaly remains clinically under-recognized. Healthcare professionals should more commonly consider acromegaly, which can lead to earlier diagnosis and better treatment outcome.
Figures
References
-
- Melmed S. Medical progress: Acromegaly. N Engl J Med. 2006;355:2558–2573. - PubMed
-
- Freda PU. Current concepts in the biochemical assessment of the patient with acromegaly. Growth Horm IGF Res. 2003;13:171–184. - PubMed
-
- Beauregard C, Truong U, Hardy J, Serri O. Long-term outcome and mortality after transsphenoidal adenomectomy for acromegaly. Clin Endocrinol (Oxf) 2003;58:86–91. - PubMed
-
- Mestron A, Webb SM, Astorga R, Benito P, Catala M, Gaztambide S, Gomez JM, Halperin I, Lucas-Morante T, Moreno B, Obiols G, de Pablos P, Paramo C, Pico A, Torres E, Varela C, Vazquez JA, Zamora J, Albareda M, Gilabert M. Epidemiology, clinical characteristics, outcome, morbidity and mortality in acromegaly based on the Spanish Acromegaly Registry (Registro Espanol de Acromegalia, REA) Eur J Endocrinol. 2004;151:439–446. - PubMed
-
- Swearingen B, Barker FG, 2nd, Katznelson L, Biller BM, Grinspoon S, Klibanski A, Moayeri N, Black PM, Zervas NT. Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab. 1998;83:3419–3426. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
