

Persistence of oxidant and protease burden in the airways after smoking cessation
- PMID: 19473482
- PMCID: PMC2697135
- DOI: 10.1186/1471-2466-9-25
Persistence of oxidant and protease burden in the airways after smoking cessation
Abstract
Background: Oxidative stress is associated with the pathogenesis of cigarette smoke related lung diseases, but longitudinal effects of smoking cessation on oxidant markers in the airways are unknown.
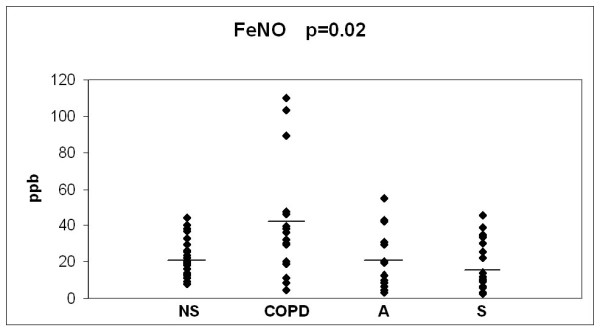
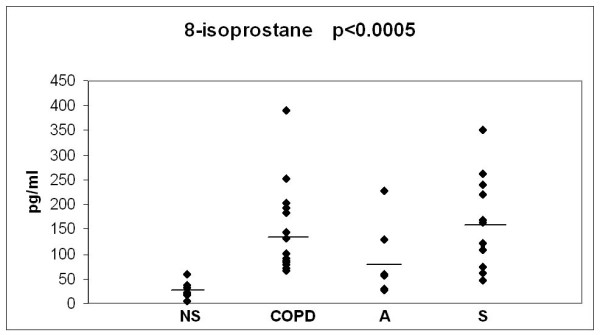
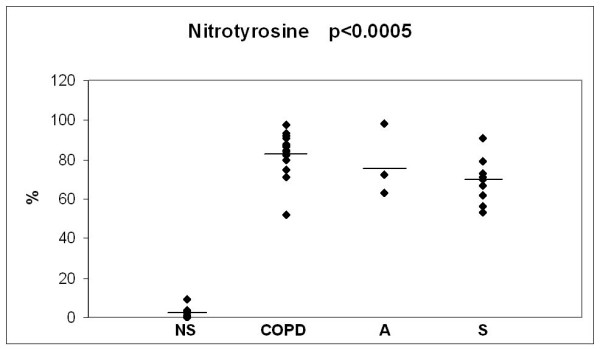
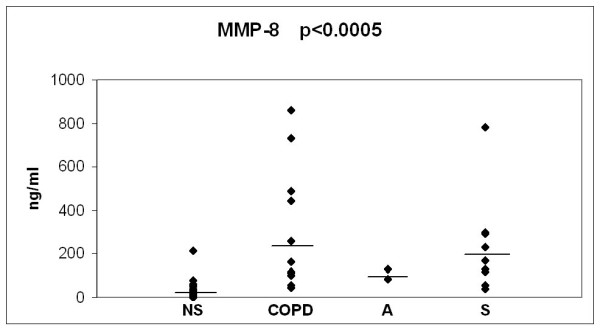
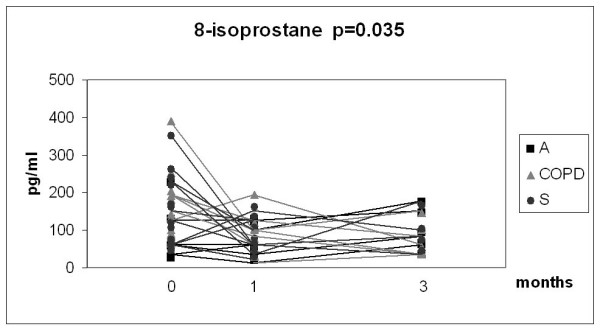
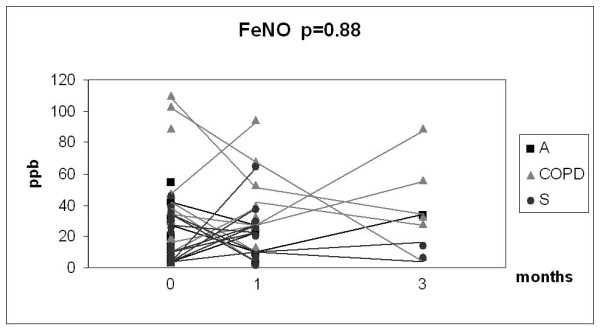
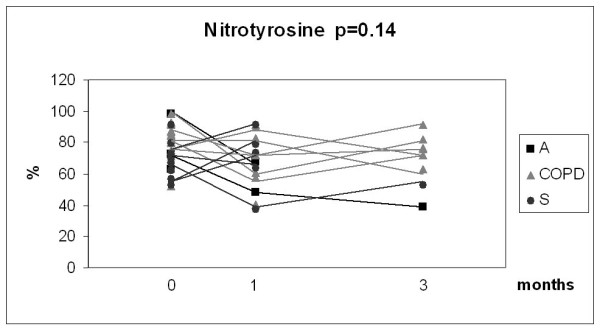
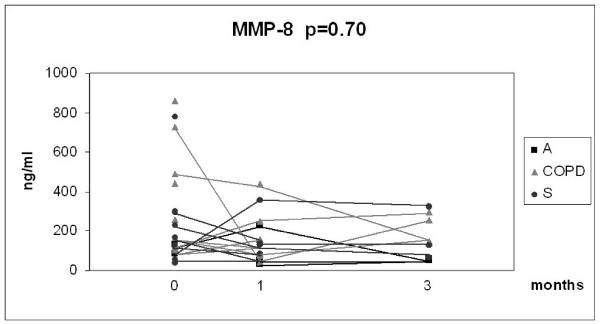
Methods: This study included 61 smokers; 21 with chronic bronchitis or COPD, 15 asthmatics and 25 asymptomatic smokers followed up for 3 months after smoking cessation. Fractional exhaled nitric oxide (FeNO), sputum neutrophil counts, sputum 8-isoprostane, nitrotyrosine and matrix metalloproteinase-8 (MMP-8) were investigated at baseline and 1 and 3 months after smoking cessation.
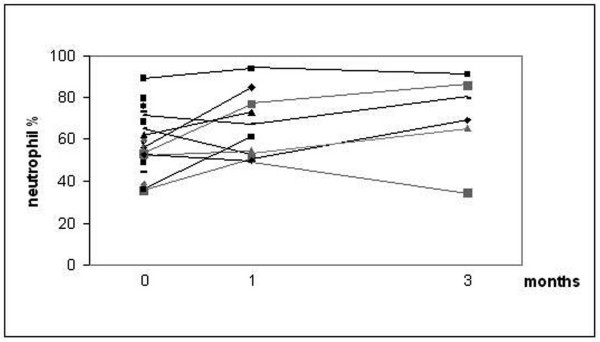
Results: After 3 months 15 subjects had succeeded in quitting of smoking and in these subjects symptoms improved significantly. Unexpectedly, however, sputum neutrophils increased (p = 0.046) after smoking cessation in patients with chronic bronchitis/COPD. At baseline, the other markers did not differ between the three groups so these results were combined for further analysis. Sputum 8-isoprostane declined significantly during the follow-up at 3 months (p = 0.035), but levels still remained significantly higher than in non-smokers. The levels of FeNO, nitrotyrosine and MMP-8 did not change significantly during the 3 months after smoking cessation.
Conclusion: Whilst symptoms improve after smoking cessation, the oxidant and protease burden in the airways continues for months.
Figures
Similar articles
-
Elevation of sputum matrix metalloproteinase-9 persists up to 6 months after smoking cessation: a research study.BMC Pulm Med. 2010 Mar 14;10:13. doi: 10.1186/1471-2466-10-13. BMC Pulm Med. 2010. PMID: 20226090 Free PMC article.
-
The acute effect of smoking in healthy and asthmatic smokers.Eur J Clin Invest. 2010 Feb;40(2):103-9. doi: 10.1111/j.1365-2362.2009.02221.x. Epub 2009 Nov 12. Eur J Clin Invest. 2010. PMID: 19912318
-
The value of sputum 8-isoprostane in detecting oxidative stress in mild asthma.J Asthma. 2008 Mar;45(2):149-54. doi: 10.1080/02770900701840261. J Asthma. 2008. PMID: 18350407
-
Airway biomarkers of the oxidant burden in asthma and chronic obstructive pulmonary disease: current and future perspectives.Int J Chron Obstruct Pulmon Dis. 2008;3(4):585-603. doi: 10.2147/copd.s3671. Int J Chron Obstruct Pulmon Dis. 2008. PMID: 19281076 Free PMC article. Review.
-
Noninvasive evaluation of airway inflammation in asthmatic patients who smoke: implications for application in clinical practice.Ann Allergy Asthma Immunol. 2008 Sep;101(3):226-32; quiz 232-4, 278. doi: 10.1016/S1081-1206(10)60485-1. Ann Allergy Asthma Immunol. 2008. PMID: 18814444 Review.
Cited by
-
[The Relationship Between Oral Microbiota and Chronic Obstructive Pulmonary Disease].Sichuan Da Xue Xue Bao Yi Xue Ban. 2023 Jan;54(1):54-60. doi: 10.12182/20230160502. Sichuan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 36647643 Free PMC article. Review. Chinese.
-
Role of Diet in Chronic Obstructive Pulmonary Disease Prevention and Treatment.Nutrients. 2019 Jun 16;11(6):1357. doi: 10.3390/nu11061357. Nutrients. 2019. PMID: 31208151 Free PMC article. Review.
-
Oxidant-antioxidant balance in the blood of patients with chronic obstructive pulmonary disease after smoking cessation.Oxid Med Cell Longev. 2013;2013:897075. doi: 10.1155/2013/897075. Epub 2013 Sep 5. Oxid Med Cell Longev. 2013. PMID: 24089631 Free PMC article.
-
Resolution of leucocyte-mediated mucosal diseases. A novel in vivo paradigm for drug development.Br J Pharmacol. 2012 Apr;165(7):2100-9. doi: 10.1111/j.1476-5381.2011.01772.x. Br J Pharmacol. 2012. PMID: 22053825 Free PMC article. Review.
-
Red blood cells protect albumin from cigarette smoke-induced oxidation.PLoS One. 2012;7(1):e29930. doi: 10.1371/journal.pone.0029930. Epub 2012 Jan 4. PLoS One. 2012. PMID: 22238677 Free PMC article.
References
-
- Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van WC, Zielinski J. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–555. doi: 10.1164/rccm.200703-456SO. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
