

Economic analysis of combined endoscopic and endobronchial ultrasound in the evaluation of patients with suspected non-small cell lung cancer
- PMID: 19473723
- PMCID: PMC2822087
- DOI: 10.1016/j.lungcan.2009.04.019
Economic analysis of combined endoscopic and endobronchial ultrasound in the evaluation of patients with suspected non-small cell lung cancer
Abstract
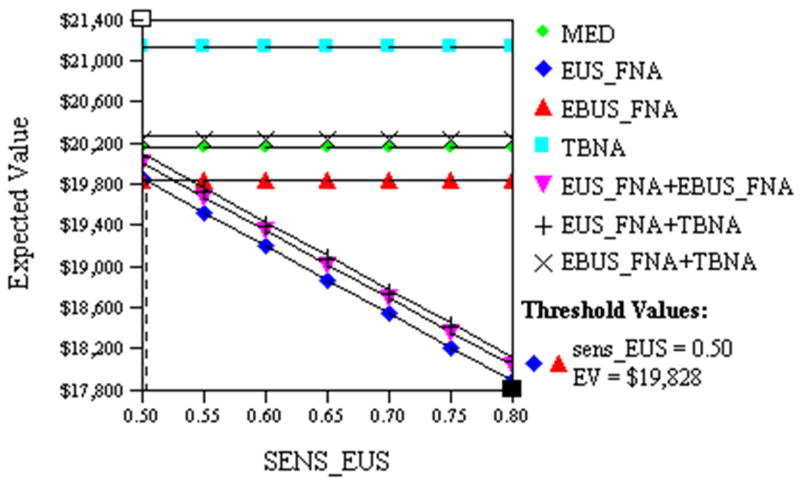
Lung cancer remains the most common cause of cancer-related death in the United States. This study evaluated the costs of alternative diagnostic evaluations for patients with suspected non-small cell lung cancer (NSCLC). Researchers used a cost-minimization model to compare various diagnostic approaches in the evaluation of patients with NSCLC. It was less expensive to use an initial endoscopic ultrasound (EUS) with fine needle aspiration (FNA) to detect a mediastinal lymph node metastasis ($18,603 per patient), compared with combined EUS FNA and endobronchial ultrasound (EBUS) with FNA ($18,753). The results were sensitive to the prevalence of malignant mediastinal lymph nodes; EUS FNA remained least costly, if the probability of nodal metastases was <32.9%, as would occur in a patient without abnormal lymph nodes on computed tomography (CT). While EUS FNA combined with EBUS FNA was the most economical approach, if the rate of nodal metastases was higher, as would be the case in patients with abnormal lymph nodes on CT. Both of these strategies were less costly than bronchoscopy or mediastinoscopy. The pre-test probability of nodal metastases can determine the most cost-effective testing strategy for evaluation of a patient with NSCLC. Pre-procedure CT may be helpful in assessing probability of mediastinal nodal metastases.
Conflict of interest statement
Figures
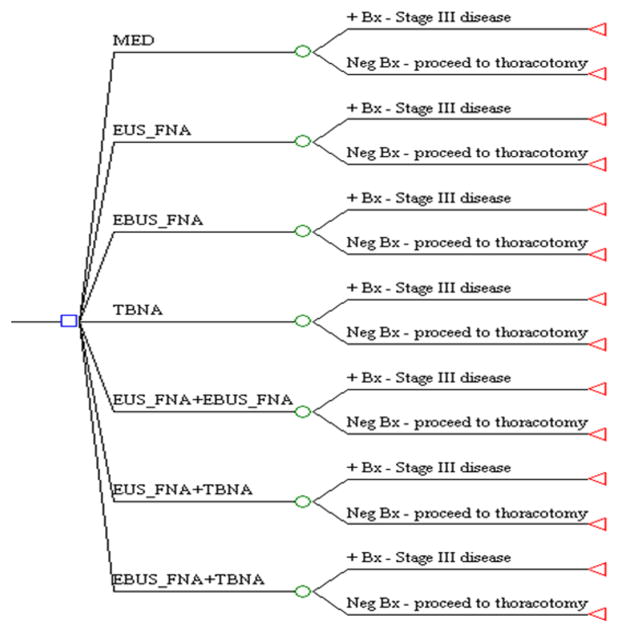
 = change node; ◃ = end of evaluation for that branch. EUS = endoscopic ultrasound; FNA = fine needle aspiration; MED = mediastinoscopy; TBNA = transbronchial needle aspiration; EBUS = endobronchial ultrasound; + Bx = biopsy yielding malignancy.
= change node; ◃ = end of evaluation for that branch. EUS = endoscopic ultrasound; FNA = fine needle aspiration; MED = mediastinoscopy; TBNA = transbronchial needle aspiration; EBUS = endobronchial ultrasound; + Bx = biopsy yielding malignancy.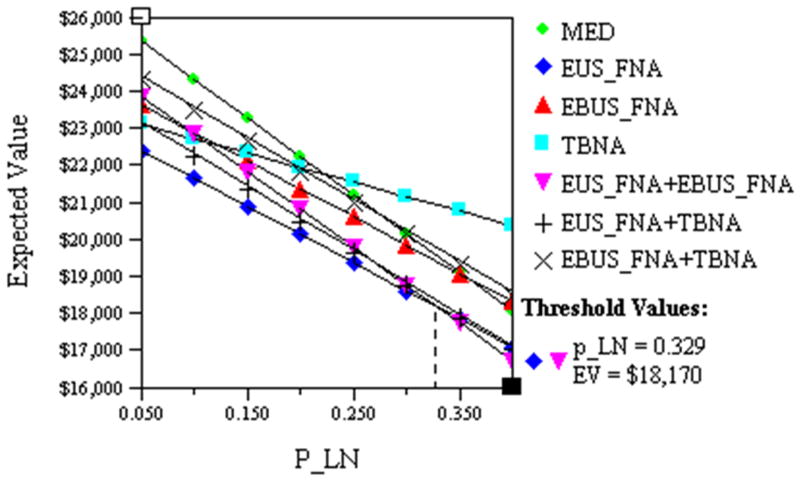
Similar articles
-
Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline, in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS).Endoscopy. 2015 Jun;47(6):545-59. doi: 10.1055/s-0034-1392040. Epub 2015 Jun 1. Endoscopy. 2015. PMID: 26030890
-
Cost-minimization analysis of alternative diagnostic approaches in a modeled patient with non-small cell lung cancer and subcarinal lymphadenopathy.Mayo Clin Proc. 2002 Feb;77(2):155-64. doi: 10.4065/77.2.155. Mayo Clin Proc. 2002. PMID: 11838649
-
Endoscopic ultrasound-guided fine-needle aspiration in patients with non-small cell lung cancer and prior negative mediastinoscopy.Ann Thorac Surg. 2005 Oct;80(4):1231-9. doi: 10.1016/j.athoracsur.2005.04.001. Ann Thorac Surg. 2005. PMID: 16181845 Clinical Trial.
-
Minimally Invasive with Maximal Yield: A Narrative Review of Current Practices in Mediastinal Lymph Node Staging in Non-Small Cell Lung Cancer.J Laparoendosc Adv Surg Tech A. 2024 Sep;34(9):773-785. doi: 10.1089/lap.2024.0138. Epub 2024 May 10. J Laparoendosc Adv Surg Tech A. 2024. PMID: 38727568 Review.
-
Choose the best route: ultrasound-guided transbronchial and transesophageal needle aspiration with echobronchoscope in the diagnosis of mediastinal and pulmonary lesions.Minerva Med. 2015 Oct;106(5 Suppl 1):13-9. Minerva Med. 2015. PMID: 27427262 Review.
Cited by
-
Endobronchial ultrasound-guided transbronchial needle aspiration combined with either endoscopic ultrasound-guided fine-needle aspiration or endoscopic ultrasound using the EBUS scope-guided fine-needle aspiration for diagnosing and staging mediastinal diseases: a systematic review and meta-analysis.Clinics (Sao Paulo). 2020 Oct 19;75:e1759. doi: 10.6061/clinics/2020/e1759. eCollection 2020. Clinics (Sao Paulo). 2020. PMID: 33084766 Free PMC article.
-
Endobronchial ultrasound-guided transbronchial needle aspiration versus mediastinoscopy for mediastinal staging of lung cancer: A systematic review of economic evaluation studies.PLoS One. 2020 Jun 30;15(6):e0235479. doi: 10.1371/journal.pone.0235479. eCollection 2020. PLoS One. 2020. PMID: 32603376 Free PMC article.
-
Balancing Accuracy, Safety, and Cost in Mediastinal Diagnostics: A Systematic Review of EBUS and Mediastinoscopy in NSCLC.Healthcare (Basel). 2025 Aug 6;13(15):1924. doi: 10.3390/healthcare13151924. Healthcare (Basel). 2025. PMID: 40805957 Free PMC article. Review.
-
Clinical efficacy and cost-effectiveness of endobronchial ultrasound-guided transbronchial needle aspiration for preoperative staging of non-small-cell lung cancer: Results of a French prospective multicenter trial (EVIEPEB).PLoS One. 2019 Jan 7;14(1):e0208992. doi: 10.1371/journal.pone.0208992. eCollection 2019. PLoS One. 2019. PMID: 30615623 Free PMC article.
-
Cost-effectiveness of endoscopic mediastinal staging.Mediastinum. 2020 Sep 30;4:18. doi: 10.21037/med-20-27. eCollection 2020. Mediastinum. 2020. PMID: 35118286 Free PMC article. Review.
References
-
- Andre F, Grunenwald D, Pignon JP, Dujon A, Pujol JL, Brichon PY, Brouchet L, Quoix E, Westeel V, Le Chevalier T. Survival of patients with resected N2 non-small-cell lung cancer: evidence for a subclassification and implications. J Clin Oncol. 2000;18:2981–2989. - PubMed
-
- Jassem J, Skokowski J, Dziadziuszko R, Jassem E, Szymanowska A, Rzyman W, Roszkiewicz A. Results of surgical treatment of non-small cell lung cancer: validation of the new postoperative pathologic TNM classification. J Thorac Cardiovasc Surg. 2000;119:1141–1146. - PubMed
-
- Okada M, Tsubota N, Yoshimura M, Miyamoto Y, Matsuoka H. How should interlobar pleural invasion be classified? Prognosis of resected T3 non-small cell lung cancer. Ann Thorac Surg. 1999;68:2049–2052. - PubMed
-
- Okada M, Tsubota N, Yoshimura M, Miyamoto Y, Matsuoka H. Prognosis of completely resected pN2 non-small cell lung carcinomas: What is the significant node that affects survival? J Thorac Cardiovasc Surg. 1999;118:270–275. - PubMed
-
- Suzuki K, Nagai K, Yoshida J, Nishimura M, Takahashi K, Nishiwaki Y. The prognosis of surgically resected N2 non-small cell lung cancer: the importance of clinical N status. J Thorac Cardiovasc Surg. 1999;118:145–153. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
