

Effect of the quality and outcomes framework on diabetes care in the United Kingdom: retrospective cohort study
- PMID: 19474024
- PMCID: PMC2687510
- DOI: 10.1136/bmj.b1870
Effect of the quality and outcomes framework on diabetes care in the United Kingdom: retrospective cohort study
Erratum in
- BMJ. 2009;339:b2768
Abstract
Objectives: To examine the management of diabetes between 2001 and 2007 in the United Kingdom and to assess whether changes in the quality of care reflect existing temporal trends or are a direct result of the implementation of the quality and outcomes framework.
Design: Retrospective cohort study.
Setting: 147 general practices (annual list size over 1 million) across the UK. Patients People with type 1 or type 2 diabetes.
Main outcome measures: Annual prevalence of diabetes and attainment of process and clinical outcomes over the three years before and the three years after the introduction of the quality and outcomes framework.
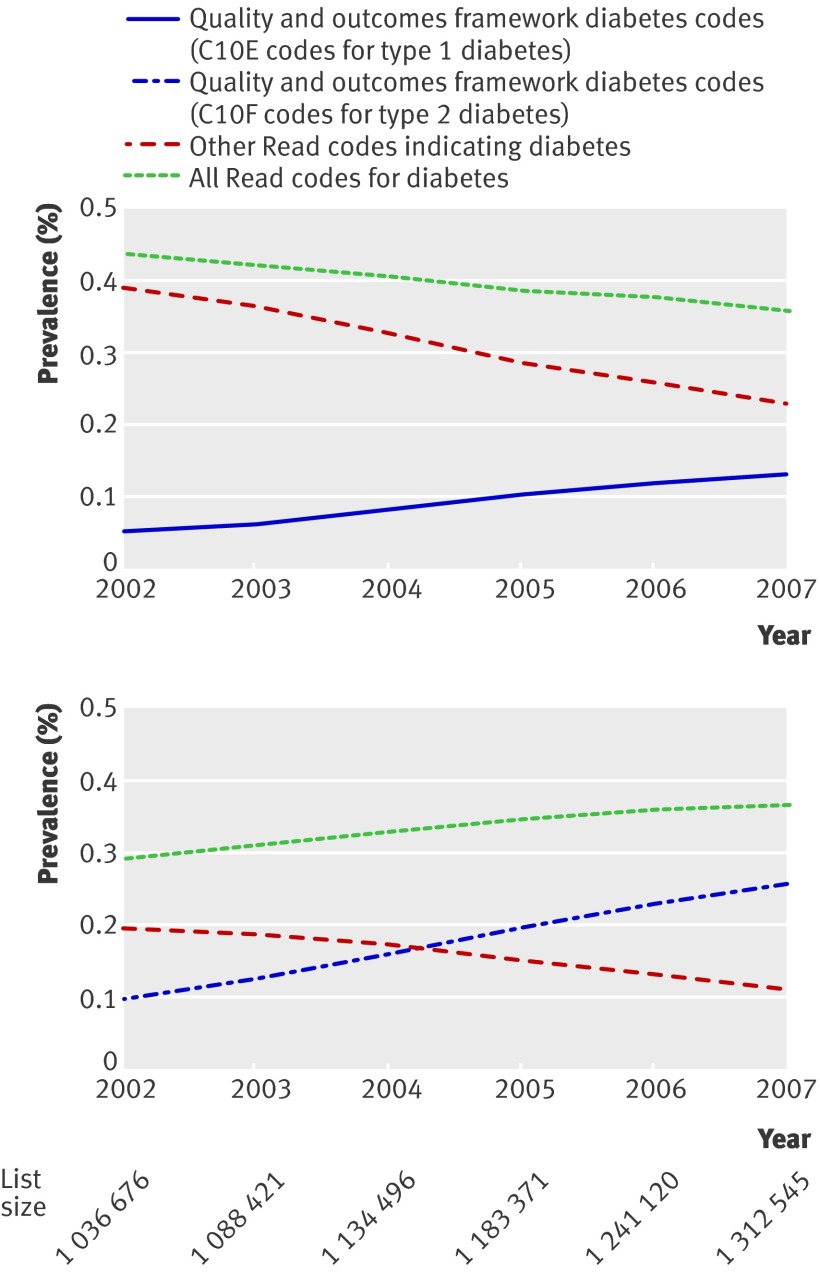
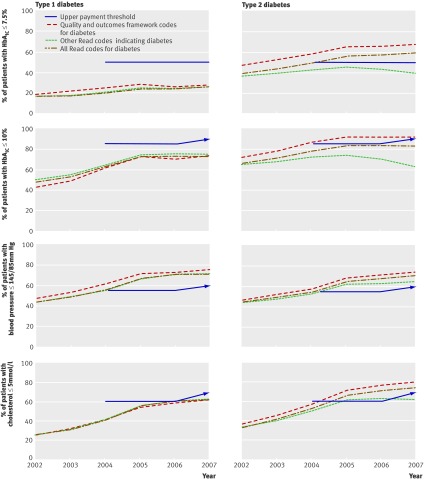
Results: Significant improvements in process and intermediate outcome measures were observed during the six year period, with consecutive annual improvements observed before the introduction of incentives. However, the current diagnostic case definition for the quality and outcomes framework does not capture up to two thirds of people with type 1 diabetes and a third of people with type 2 diabetes. After the introduction of the quality and outcomes framework, existing trends of improvement in glycaemic control, cholesterol levels, and blood pressure were attenuated, particularly in people with diabetes who did not meet the case definition of the quality and outcomes framework. The introduction of the quality and outcomes framework did not lead to improvement in the management of patients with type 1 diabetes, nor to a reduction in the number of patients with type 2 diabetes who had HbA(1c) levels greater than 10%. Introduction of the quality and outcomes framework may have increased the number of patients with type 2 diabetes with HbA(1c) levels of <or=7.5%; odds ratio 1.05 (95% confidence interval 1.01 to 1.09; P=0.02).
Conclusions: The management of people with diabetes has improved since the late 1990s, but the impact of the quality and outcomes framework on care is not straightforward; upper thresholds may need to be removed or targets made more challenging if people are to benefit. Many patients in whom care may be suboptimal may not be captured in the quality and outcomes framework assessment.
Conflict of interest statement
Competing interests: MJC, AS, RJM, and NF have received funding for research, consulting, and travel from several companies that manufacture therapies for diabetes.
Figures
References
-
- Institute of Medicine. Rewarding provider performance: aligning incentives in Medicare. Washington: National Academies Press, 2007.
-
- Roland M. Linking physician pay to quality of care: a major experiment in the United Kingdom. N Engl J Med 2004;351:1448-54. - PubMed
-
- Royal College Of General Practitioners. The GMS contract (overview and resources guide). London 2007. www.rcgp.org.uk/pdf/ISS_INFO_GMS07.pdf.
-
- British Medical Association 2009. www.bma.org.uk/employmentandcontracts/independent_contractors/quality_ou....
-
- Doran T, Fullwood C, Reeves D, Gravelle H, Roland M. Exclusion of patients from pay-for-performance targets by English physicians. N Engl J Med 2008;359:274-84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous