

Reducing the prescribing of heavily marketed medications: a randomized controlled trial
- PMID: 19475459
- PMCID: PMC2710467
- DOI: 10.1007/s11606-009-1013-x
Reducing the prescribing of heavily marketed medications: a randomized controlled trial
Abstract
Context: Prescription drug costs are a major component of health care expenditures, yet resources to support evidence-based prescribing are not widely available.
Objective: To evaluate the effectiveness of computerized prescribing alerts, with or without physician-led group educational sessions, to reduce the prescribing of heavily marketed hypnotic medications.
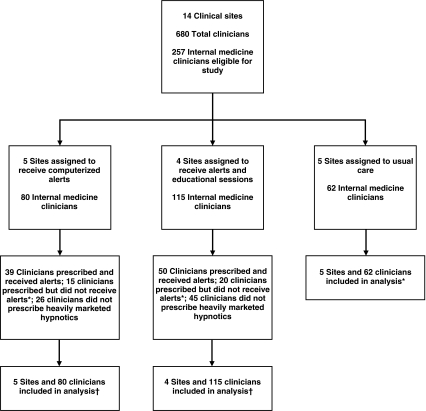
Design: Cluster-randomized controlled trial.
Setting: We randomly allocated 14 internal medicine practice sites to receive usual care, computerized prescribing alerts alone, or alerts plus group educational sessions.
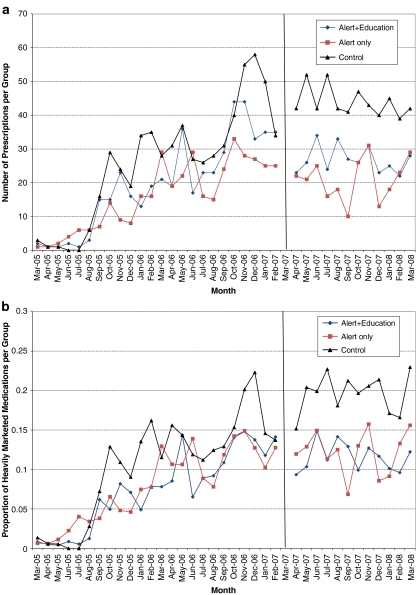
Measurements: Proportion of heavily marketed hypnotics prescribed before and after the implementation of computerized alerts and educational sessions.
Main results: The activation of computerized alerts held the prescribing of heavily marketed hypnotic medications at pre-intervention levels in both the alert-only group (adjusted risk ratio [RR] 0.97; 95% CI 0.82-1.14) and the alert-plus-education group (RR 0.98; 95% CI 0.83-1.17) while the usual-care group experienced an increase in prescribing (RR 1.31; 95% CI 1.08-1.60). Compared to the usual-care group, the relative risk of prescribing heavily marketed medications was less in both the alert-group (Ratio of risk ratios [RRR] 0.74; 95% CI 0.57-0.96) and the alert-plus-education group (RRR 0.74; 95% CI 0.58-0.97). The prescribing of heavily marketed medications was similar in the alert-group and alert-plus-education group (RRR 1.02; 95% CI 0.80-1.29). Most clinicians reported that the alerts provided useful prescribing information (88%) and did not interfere with daily workflow (70%).
Conclusions: Computerized decision support is an effective tool to reduce the prescribing of heavily marketed hypnotic medications in ambulatory care settings.
Trial registration: clinicaltrials.gov Identifier: NCT00788346.
Figures
References
-
- Center for Medicare & Medicaid Services. National Health Expenditure Accounts 2006 Highlights. http://www.cms.hhs.gov/NationalHealthExpendData/downloads/highlights.pdf. 2006. Accessed April 21, 2009.
-
- US Government Accountability Office. Prescription Drugs: Improvements Needed in FDA's Oversight of Direct-to-Consumer Advertising (GAO-07–54). 11–16–0008.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
