

Amyloid imaging in mild cognitive impairment subtypes
- PMID: 19475670
- PMCID: PMC2828870
- DOI: 10.1002/ana.21598
Amyloid imaging in mild cognitive impairment subtypes
Erratum in
- Ann Neurol. 2009 Jul;66(1):123. DeKoskym, Steven T [corrected to De-Kosky, Steven T]
Abstract
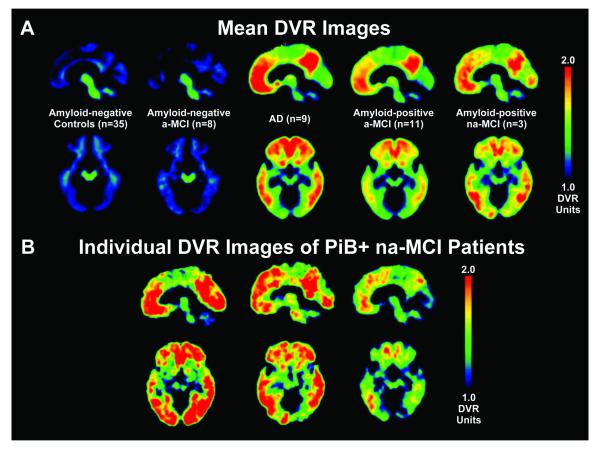
Objective: We utilized the amyloid imaging ligand Pittsburgh Compound B (PiB) to determine the presence of Alzheimer's disease (AD) pathology in different mild cognitive impairment (MCI) subtypes and to relate increased PiB binding to other markers of early AD and longitudinal outcome.
Methods: Twenty-six patients with MCI (13 single-domain amnestic-MCI [a-MCI], 6 multidomain a-MCI, and 7 nonamnestic MCI) underwent PiB imaging. Twenty-three had clinical follow-up (21.2 +/- 16.0 [standard deviation] months) subsequent to their PiB scan.
Results: Using cutoffs established from a control cohort, we found that 14 (54%) patients had increased levels of PiB retention and were considered "amyloid-positive." All subtypes were associated with a significant proportion of amyloid-positive patients (6/13 single-domain a-MCI, 5/6 multidomain a-MCI, 3/7 nonamnestic MCI). There were no obvious differences in the distribution of PiB retention in the nonamnestic MCI group. Predictors of conversion to clinical AD in a-MCI, including poorer episodic memory, and medial temporal atrophy, were found in the amyloid-positive relative to amyloid-negative a-MCI patients. Longitudinal follow-up demonstrated 5 of 13 amyloid-positive patients, but 0 of 10 amyloid-negative patients, converted to clinical AD. Further, 3 of 10 amyloid-negative patients "reverted to normal."
Interpretation: These data support the notion that amyloid-positive patients are likely to have early AD, and that the use of amyloid imaging may have an important role in determining which patients are likely to benefit from disease-specific therapies. In addition, our data are consistent with longitudinal studies that suggest a significant percentage of all MCI subtypes will develop AD.
Figures




References
-
- Petersen RC. Mild cognitive impairment as a diagnostic entity. Journal of Internal Medicine. 2004;256:183–194. - PubMed
-
- Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–246. - PubMed
-
- Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch Neurol. 2001;58:397–405. - PubMed
-
- Petersen RC, Smith GE, Waring SC, et al. Mild cognitive impairment. Clinical characterization and outcome. Archives of Neurology. 1999;56:303–308. - PubMed
-
- Feldman H, Scheltens P, Scarpini E, et al. Behavioral symptoms in mild cognitive impairment. Neurology. 2004;62:1199–1201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG 020226/AG/NIA NIH HHS/United States
- K23 AG 028018/AG/NIA NIH HHS/United States
- R01 AG018402/AG/NIA NIH HHS/United States
- P50 AG 005133/AG/NIA NIH HHS/United States
- R01 MH070729/MH/NIMH NIH HHS/United States
- R37 AG025516/AG/NIA NIH HHS/United States
- R01 AG 018402/AG/NIA NIH HHS/United States
- R01 AG020226/AG/NIA NIH HHS/United States
- R01 AG 020098/AG/NIA NIH HHS/United States
- K01 MH001976/MH/NIMH NIH HHS/United States
- R01 MH 070729/MH/NIMH NIH HHS/United States
- K02 AG 001039/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- K02 AG 027998/AG/NIA NIH HHS/United States
- P01 AG 025204/AG/NIA NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- RF1 AG025516/AG/NIA NIH HHS/United States
- K02 AG001039/AG/NIA NIH HHS/United States
- R37 AG 025516/AG/NIA NIH HHS/United States
- K23 AG028018/AG/NIA NIH HHS/United States
- P01 AG025204/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
