

Remission of epilepsy after two drug failures in children: a prospective study
- PMID: 19475671
- PMCID: PMC2818062
- DOI: 10.1002/ana.21642
Remission of epilepsy after two drug failures in children: a prospective study
Abstract
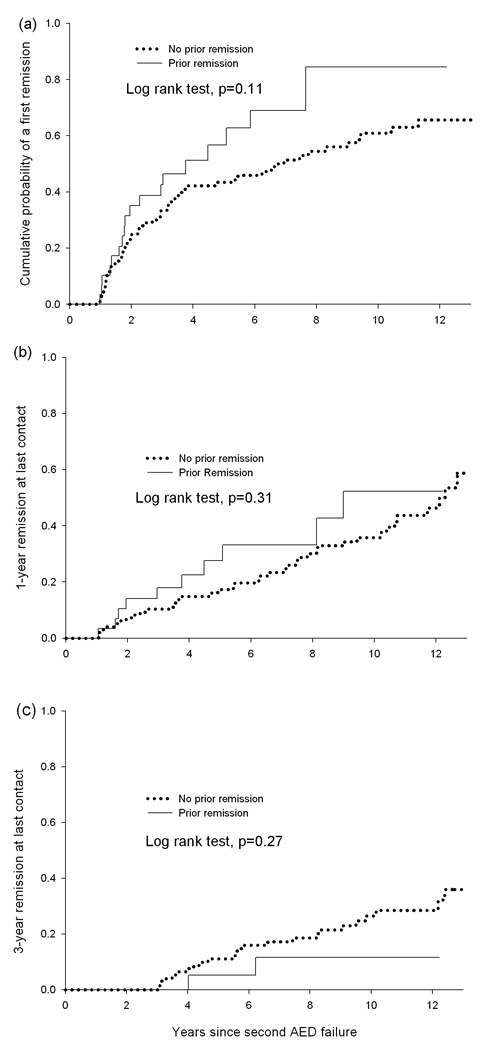
Objective: Determine the probability of a more than 1-year remission after failure of a second drug in children prospectively followed from initial diagnosis of epilepsy and then from time of second drug failure. Identify prognostic factors for remission after second drug failure.
Methods: Of 613 children, 128 did not respond favorably to 2 drugs, had a trial of at least a third drug (median, 3), and were followed for more than 1 year (median, 10.1 years) since second drug failure. Product limit and proportional hazards techniques were used to analyze predictors of any 1-year remission (Rem1) and 1- and 3-year remission at last contact (Rem1/3-LC).
Results: Seventy-three patients (57%) had a remission. Repeated remissions and relapses were common. Only 48 (37.5%) achieved Rem1-LC and 28 (23%) Rem3-LC. Idiopathic epilepsy (Rem1: rate ratio [RR], 3.64, p < 0.0001; Rem1-LC: RR, 2.57, p = 0.008) and seizure frequency (Rem1: RR, 0.76, p = 0.003; Rem1-LC: RR, 0.82, p = 0.04 per increase in category) were the most robust predictors. Symptomatic cause was the only correlate of Rem3-LC. Remission before second drug failure did not predict remission after second drug failure.
Interpretation: Remission after second drug failure is common but often temporary. Children who have not responded to two appropriate drugs should be carefully evaluated to maximize therapy and possibly considered for more aggressive treatments.
Figures

Comment in
-
Is the epilepsy responsive or resistant? Only time will tell.Ann Neurol. 2009 May;65(5):489-90. doi: 10.1002/ana.21679. Ann Neurol. 2009. PMID: 19479723 No abstract available.
-
What is intractable epilepsy, and when (if ever) does it remit with medical treatment?Curr Neurol Neurosci Rep. 2010 Jul;10(4):249-51. doi: 10.1007/s11910-010-0115-5. Curr Neurol Neurosci Rep. 2010. PMID: 20454873 No abstract available.
References
-
- Dlugos D, Sammel M, Strom B, Farrar J. Response to first drug trial predicts outcome in childhood temporal lobe epilepsy. Neurology. 2001;57:2259–2264. - PubMed
-
- Camfield P, Camfield C. Nova Scotia pediatric epilepsy study. In: Jallon P, Berg A, Dulac O, Hauser A, editors. Prognosis of epilepsies. Montrouge France: John Libbey, Eurotext; 2003. pp. 113–126.
-
- Arts WFM, Brouwer OF, Peters ACB, et al. Course and prognosis of childhood epilepsy: 5-year follow-up of the Dutch study of epilepsy in childhood. Brain. 2004;127:1774–1784. - PubMed
-
- Berg AT, Vickrey BG, Testa FM, et al. How long does it take epilepsy to become intractable? A prospective investigation. Ann Neurol. 2006;60:73–79. - PubMed
-
- Spooner CG, Berkovic SF, Mitchell LA, et al. New onset temporal lobe epilepsy in children: lesion on MRI predicts poor seizure outcome. Neurology. 2006;67:2147–2153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
