

Use of helical CT is associated with an increased incidence of postoperative pulmonary emboli in cancer patients with no change in the number of fatal pulmonary emboli
- PMID: 19476851
- PMCID: PMC6351075
- DOI: 10.1016/j.jamcollsurg.2008.12.030
Use of helical CT is associated with an increased incidence of postoperative pulmonary emboli in cancer patients with no change in the number of fatal pulmonary emboli
Abstract
Background: Multidetector computed tomography (MDCT) scanning technology has increased the ease with which pulmonary emboli (PE) are evaluated. Our aim was to determine whether the incidence and severity of postoperative PE have changed since adoption of multidetector computed tomography.
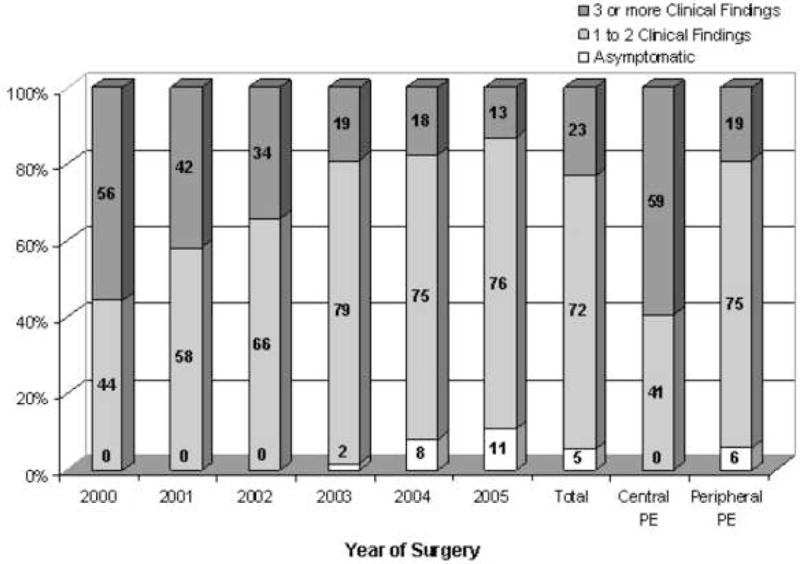
Study design: A prospective postoperative morbidity and mortality database from a single institution was used to identify all cancer patients who experienced a PE within 30 days of thoracic, abdominal, or pelvic operations. The incidence, type (central, segmental, and subsegmental), and severity of PE were examined.
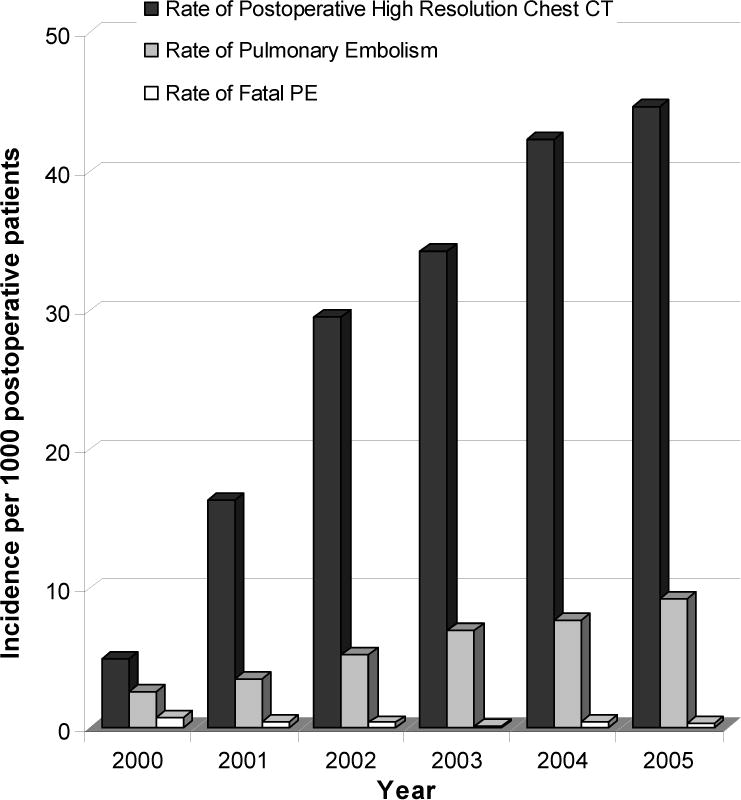
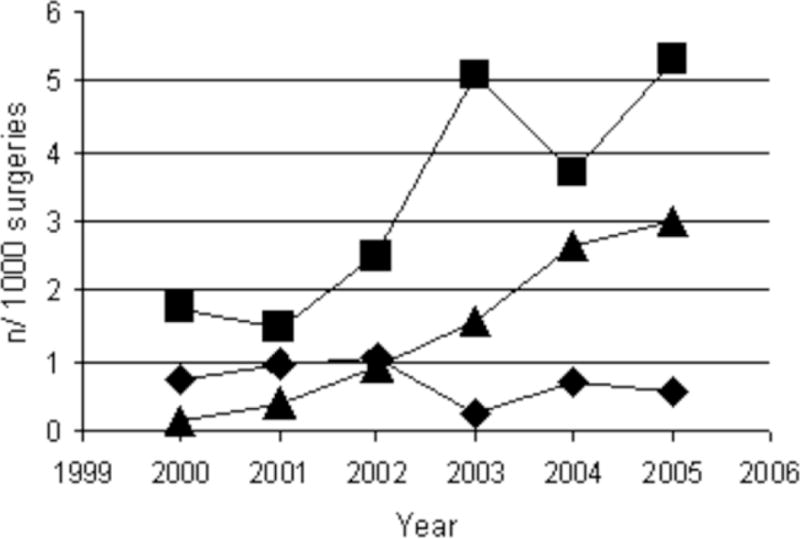
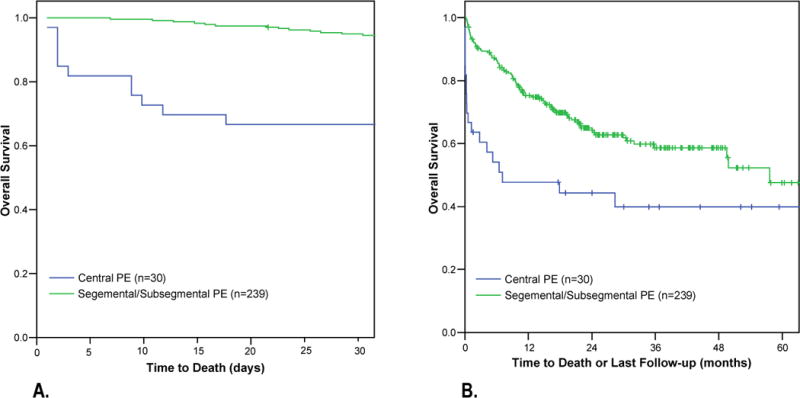
Results: A total of 295 PE were documented among 47,601 postoperative cancer patients. The incidence of PE increased yearly from 2.3 per 1,000 patients in 2000 to 9.3 per 1,000 patients in 2005 (p < 0.0001). This corresponded to an increasing number of CT scans of the chest performed (6.6 CT scans per 1,000 postoperative patients in 2000 versus 45 in 2005; p < 0.0001). The increased incidence was because of a 7.8% (CI, 4.0 to 11.7) and 5.4% (CI, 4.1 to 6.7) average annual increase in segmental and subsegmental PE, respectively. There was no change in the number of central (0.1%; CI, -1.0 to 1.12) PE. Overall incidence of fatal PE was 0.4 and did not change during the time period (p = 0.3). A central PE was more commonly associated with hypoxia, ICU admission, and 30-day mortality (33% versus 5% for peripheral; p = 0.02).
Conclusions: Chest CT scans are being performed more frequently on postoperative cancer patients and have resulted in an increased diagnosis of peripheral PE. The clinical significance of, and optimal treatment for, diagnosed subsegmental PE are incompletely defined.
Figures
References
-
- Kakkar AK, Haas S, Wolf H, Encke A. Evaluation of perioperative fatal pulmonary embolism and death in cancer surgical patients: the MC-4 cancer substudy. Thromb Haemost. 2005;94:867–871. - PubMed
-
- van Belle A, Buller HR, Huisman MV, et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295:172–179. - PubMed
-
- Raptopoulos V, Boiselle PM. Multi-detector row spiral CT pulmonary angiography: comparison with single-detector row spiral CT. Radiology. 2001;221:606–613. - PubMed
-
- Quiroz R, Kucher N, Zou KH, et al. Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review. JAMA. 2005;293:2012–2017. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
