

Comparison of phantom and registration scaling corrections using the ADNI cohort
- PMID: 19477282
- PMCID: PMC2800076
- DOI: 10.1016/j.neuroimage.2009.05.045
Comparison of phantom and registration scaling corrections using the ADNI cohort
Abstract
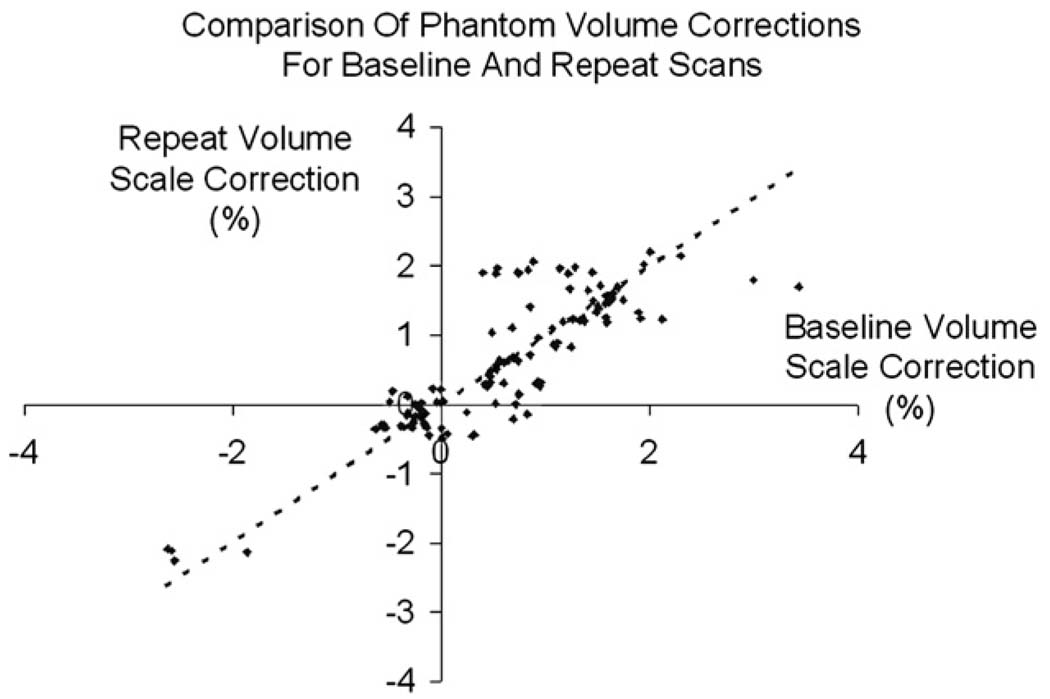
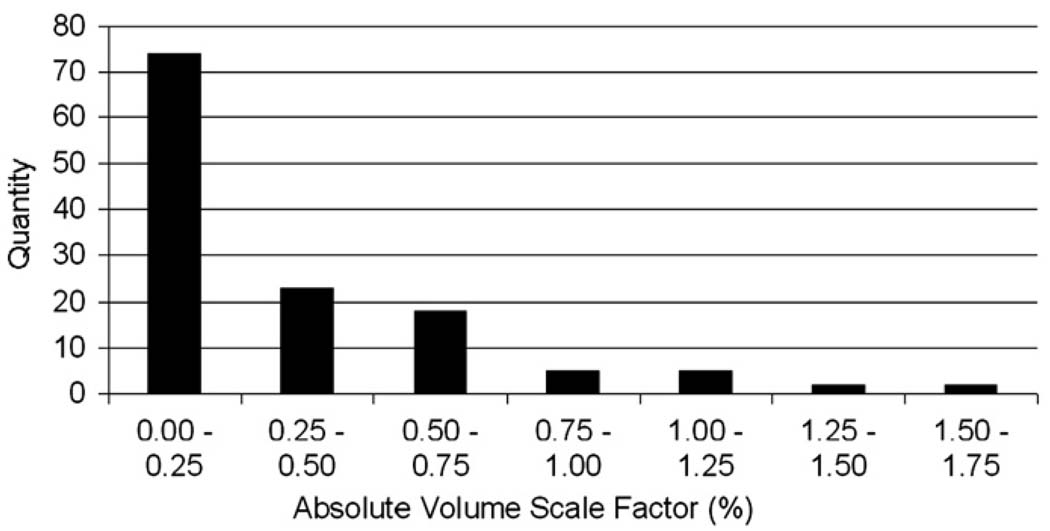
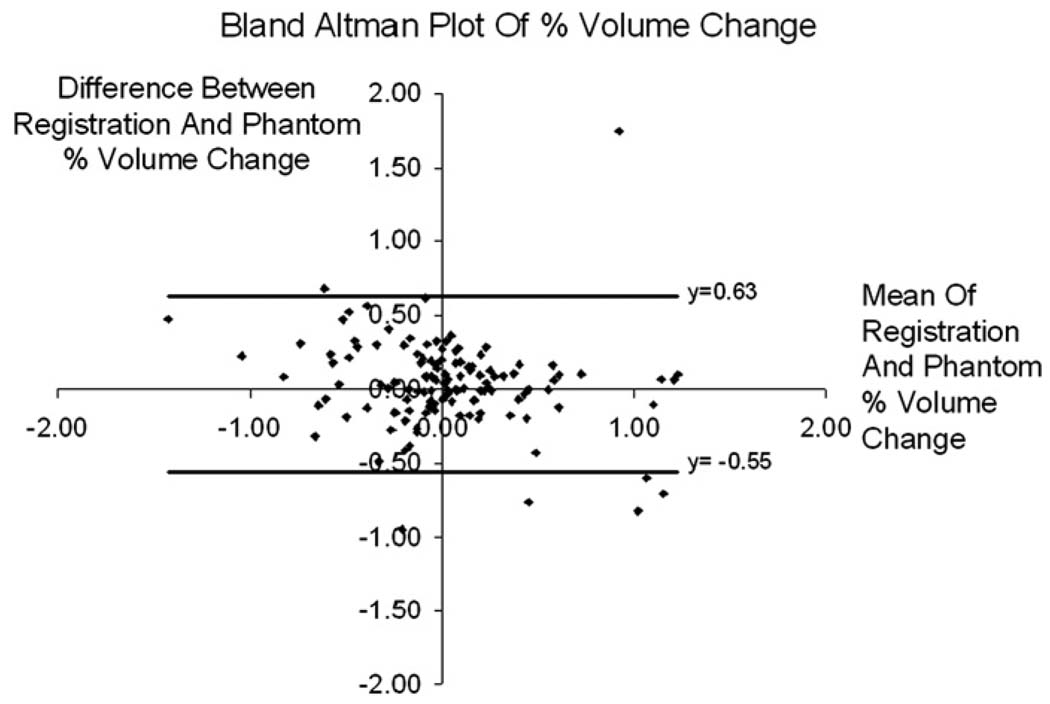
Rates of brain atrophy derived from serial magnetic resonance (MR) studies may be used to assess therapies for Alzheimer's disease (AD). These measures may be confounded by changes in scanner voxel sizes. For this reason, the Alzheimer's Disease Neuroimaging Initiative (ADNI) included the imaging of a geometric phantom with every scan. This study compares voxel scaling correction using a phantom with correction using a 9 degrees of freedom (9DOF) registration algorithm. We took 129 pairs of baseline and 1-year repeat scans, and calculated the volume scaling correction, previously measured using the phantom. We used the registration algorithm to quantify any residual scaling errors, and found the algorithm to be unbiased, with no significant (p=0.97) difference between control (n=79) and AD subjects (n=50), but with a mean (SD) absolute volume change of 0.20 (0.20) % due to linear scalings. 9DOF registration was shown to be comparable to geometric phantom correction in terms of the effect on atrophy measurement and unbiased with respect to disease status. These results suggest that the additional expense and logistic effort of scanning a phantom with every patient scan can be avoided by registration-based scaling correction. Furthermore, based upon the atrophy rates in the AD subjects in this study, sample size requirements would be approximately 10-12% lower with (either) correction for voxel scaling than if no correction was used.
Figures
References
-
- Archer HA, Edison P, Brooks DJ, Barnes J, Frost C, Yeatman T, Fox NC, Rossor MN. Amyloid load and cerebral atrophy in Alzheimer's disease: an 11C-PIB positron emission tomography study. Ann. Neurol. 2006 Jul;60(1):145–147. - PubMed
-
- Braak H, Braak E. Staging of Alzheimer's disease-related neurofibrillary changes. Neurobiol. Aging. 1995;16(3):271–278. discussion 278–84. - PubMed
-
- MarCarlson NE, Moore MM, Dame A, Howieson D, Silbert LC, Quinn JF, Kaye JA. Trajectories of brain loss in aging and the development of cognitive impairment. Neurology. 2008;70(11):828–833. - PubMed
-
- Chan D, Janssen JC, Whitwell JL, Watt HC, Jenkins R, Frost C, Rossor MN, Fox NC. Change in rates of cerebral atrophy over time in early-onset Alzheimer's disease: longitudinal MRI study. Lancet. 2003 Oct;362(9390):1121–1122. - PubMed
-
- Evans MC, Nielsen C, Douiri A, Barnes J, Clegg SL, Lehmann M, Mellow T, McNaught E, Ahsan L, Boyes R, Pepple T, Foster J, Rosser MN, Fox N. Automating the BSI brain atrophy rate calculation: comparison of using automated and semi-automated brain regions. Alzheimer's Dement. 2008 July;4(4) Supplement 1:T84–T85.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
