

Autoantibodies to a 140-kd protein in juvenile dermatomyositis are associated with calcinosis
- PMID: 19479859
- PMCID: PMC2701555
- DOI: 10.1002/art.24547
Autoantibodies to a 140-kd protein in juvenile dermatomyositis are associated with calcinosis
Abstract
Objective: The identification of novel autoantibodies in juvenile dermatomyositis (DM) may have etiologic and clinical implications. The aim of this study was to describe autoantibodies to a 140-kd protein in children recruited to the Juvenile DM National Registry and Repository for UK and Ireland.
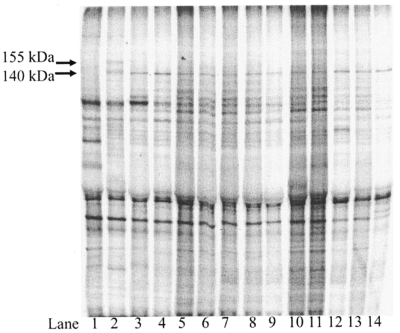
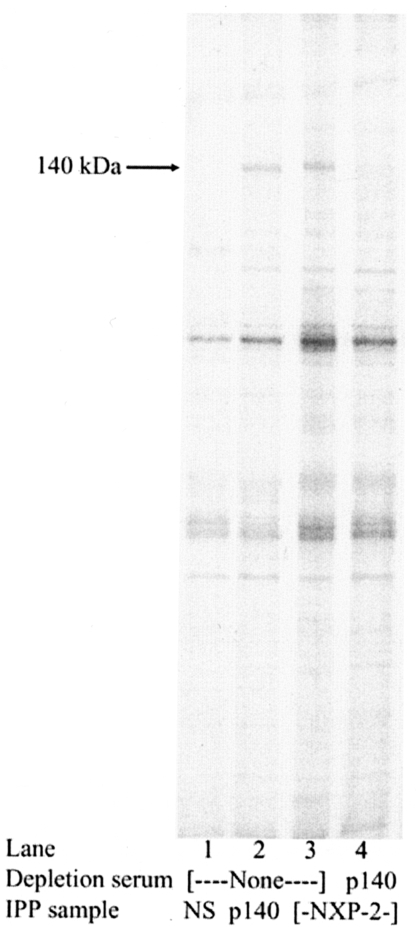
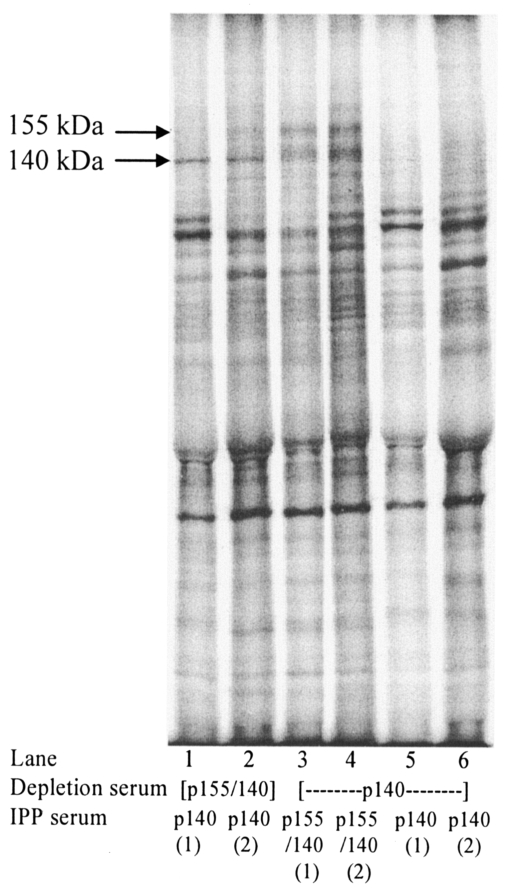
Methods: Clinical data and sera were collected from children with juvenile myositis. Sera that recognized a 140-kd protein by immunoprecipitation were identified. The identity of the p140 autoantigen was investigated by immunoprecipitation/immunodepletion, using commercial monoclonal antibodies to NXP-2, reference anti-p140, and anti-p155/140, the other autoantibody recently described in juvenile DM. DNA samples from 100 Caucasian children with myositis were genotyped for HLA class II haplotype associations and compared with those from 864 randomly selected UK Caucasian control subjects.
Results: Sera from 37 (23%) of 162 patients with juvenile myositis were positive for anti-p140 autoantibodies, which were detected exclusively in patients with juvenile DM and not in patients with juvenile DM-overlap syndrome or control subjects. No anti-p140 antibody-positive patients were positive for other recognized autoantibodies. Immunodepletion suggested that the identity of p140 was consistent with NXP-2 (the previously identified MJ autoantigen). In children with anti-p140 antibodies, the association with calcinosis was significant compared with the rest of the cohort (corrected P < 0.005, odds ratio 7.0, 95% confidence interval 3.0-16.1). The clinical features of patients with anti-p140 autoantibodies were different from those of children with anti-p155/140 autoantibodies. The presence of HLA-DRB1*08 was a possible risk factor for anti-p140 autoantibody positivity.
Conclusion: This study has established that anti-p140 autoantibodies represent a major autoantibody subset in juvenile DM. This specificity may identify a further immunogenetic and clinical phenotype within the juvenile myositis spectrum that includes an association with calcinosis.
Figures
References
-
- Mendez EP, Lipton R, Ramsey-Goldman R, Roettcher P, Bowyer S, Dyer A, et al. for the NIAMS Juvenile DM Registry Physician Referral Group US incidence of juvenile dermatomyositis, 1995–1998: results from the National Institute of Arthritis and Musculoskeletal and Skin Diseases Registry. Arthritis Rheum. 2003;49:300–5. - PubMed
-
- Oddis CV, Conte CG, Steen VD, Medsger TA., Jr. Incidence of polymyositis-dermatomyositis: a 20-year study of hospital diagnosed cases in Allegheny County, PA 1963-1982. J Rheumatol. 1990;17:1329–34. - PubMed
-
- Symmons DP, Sills JA, Davis SM. The incidence of juvenile dermatomyositis: results from a nation-wide study. Br J Rheumatol. 1995;34:732–6. - PubMed
-
- Huber AM, Lang B, LeBlanc CM, Birdi N, Bolaria RK, Malleson P, et al. Medium- and long-term functional outcomes in a multicenter cohort of children with juvenile dermatomyositis. Arthritis Rheum. 2000;43:541–9. - PubMed
-
- Ramanan AV, Feldman BM. Clinical features and outcomes of juvenile dermatomyositis and other childhood onset myositis syndromes. Rheum Dis Clin North Am. 2002;28:833–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
